BPH BPH
(Benign Prostatic (Benign Prostatic
Hyperplasia) Hyperplasia)
Presented by: Presented by:
Diana M. Diana M. Resultay Resultay
Group 3B Group 3B- - 301 301
ntroduction ntroduction
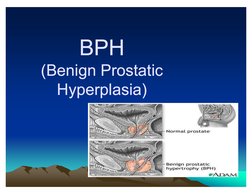
The prostate is the genital organ most commonly affected by benign and
malignant neoplasm. Benign enlargement of the prostate gland is an
extremely common process that occurs in nearly all men with functioning
testes. Hyperplasia is a general medical term referring to excess cell
replication. Benign prostatic hyperplasia (BPH) is a noncancerous growth
of the prostate gland. t is the most common noncancerous form of cell
growth in men and usually begins with microscopic nodules in younger
men. t should be noted that BPH is not a precancerous condition.
Some studies have suggested that African American men are at higher
risk and Asian men at lower risk for BPH than Caucasians, a 2000 study
found no greater risk for African Americans and only a slightly lower risk
for Asians. Among Caucasians in the study, men of southern European
heritage were at greater risk while men of Scandinavian ancestry had a
lower chance of developing BPH.
W Histologic evidence of prostate enlargement
begins about the third decade of life and
increases proportionally with aging. Specifically,
about 43% of men in their 40s will have evidence
of BPH, as will 50% of men in their 50s, 75% to
88% in their 80s, and nearly 100% of men
reaching the ninth decade of life.
W Some evidence has reported a higher incidence
of benign prostatic hyperplasia -- particularly fast-
growing BPH -- in men with obesity, heart and
circulatory diseases, and type 2 diabetes.
Diabetes and hypertension, in any case, worsens
urinary tract symptoms in men with BPH. n one
study, flow rates were adversely affected by
diabetes, although residual urine volumes were
not significantly greater.
The exact cause of BPH is unknown. Potential risk factors include age, family The exact cause of BPH is unknown. Potential risk factors include age, family
history, race, ethnicity, and hormonal factors. Androgens (male hormones) most history, race, ethnicity, and hormonal factors. Androgens (male hormones) most
likely play a role in prostate growth. The most important androgen likely play a role in prostate growth. The most important androgen
istestosterone, which is produced throughout a man's lifetime. The prostate istestosterone, which is produced throughout a man's lifetime. The prostate
converts testosterone to a more powerful androgen, dihydrotestosterone(DHT). converts testosterone to a more powerful androgen, dihydrotestosterone(DHT).
DHT stimulates cell growth in the tissue that lines the prostate gland (the DHT stimulates cell growth in the tissue that lines the prostate gland (the
glandular epithelium) and is the major cause of the rapid prostate enlargement glandular epithelium) and is the major cause of the rapid prostate enlargement
that occurs between puberty and young adulthood. DHT is a prime suspect in that occurs between puberty and young adulthood. DHT is a prime suspect in
prostate enlargement in later adulthood. Additional factors also include a prostate enlargement in later adulthood. Additional factors also include a
defective cell death in which cells naturally self defective cell death in which cells naturally self--destruct, goes awry and results destruct, goes awry and results
in cell proliferation a process called asapoptosis. in cell proliferation a process called asapoptosis.
W As BPH progresses, overgrowth occurs in the central
area of the prostate called the transition zone, which
wraps around the urethra (the tube that carries urine
through the penis). This pressure on the urethra can
cause lower urinary symptoms that have been the basis
for diagnosing BPH. t should be noted that BPH is not
always the cause of these symptoms. An enlarged
prostate may be accompanied by few symptoms, while
severe LUTS may be present with normal or even small
prostates and are most likely due to other conditions.
Symptoms of BPH may include;Difficulty in starting to
pass
W urine (hesitancy), a weak stream of urine, dribbling after
urinating, the need to strain to pass urine, incomplete
emptying of bladder, difficulty to control the urination
urge, having to get up several times in the night to pass
urine, feeling a burning sensation when passing urine.
W Sometimes a man is unaware of an obstruction until he
suddenly cannot urinate at all. This condition is called
acute urinary retention. t is a dangerous complication that
can damage the kidneys and may require emergency
surgery. n general, BPH progresses very slowly and
acute urinary retention is very uncommon. Men with BPH
at highest risk for this complication tend to be elderly and
to have moderate to severe lower voiding symptoms.
Taking anti- hypertensive drugs (except for diuretics) or
antiarrhythmic drugs may also increase the risk. Bladder
obstruction can also cause bladder stones, blood in the
urine, urinary tract infection, and incontinence.
Unfortunately, no current tests can accurately predict
which men are at higher risk for complications, although
men with a weak urine stream and larger prostates are at
higher risk for urinary retention.
W Diagnostic tests used to confirm Benign
Prostatic Hyperplasia include Digital Rectal
W Exam, Urinalysis, Serum Creatinine,
Postvoid Residual Urine, Ultrasound,
Urethrocystoscope
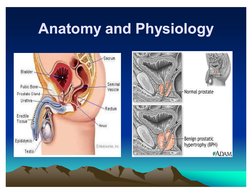
Anatomy and PhysioIogy Anatomy and PhysioIogy
W The prostate gland is located under the urinary
bladder, in front of the rectum and wraps around
the urethra (the tube that carries urine through
the penis). t is basically composed of three
different cell types the glandular cells, smooth
muscle cells and stromal cells
W The central area of the prostate that wraps
around the urethra is called the transition zone.
W The entire prostate gland is surrounded by a
dense, fibrous capsule.
W The prostate gland provides the following
functions: (1) the glandular cells produce a milky
fluid, and during sex the smooth muscles
contract and squeeze this fluid into the urethra.
Here, it mixes with sperm and other fluids to
make semen. (2) the prostate also secretes
another substance that may have antibacterial
properties. (3) the prostate gland also contains
an enzyme called 5 alpha-reductase that
converts testosterone to dihydrotestosterone,
another male hormone that has a major impact
on the prostate.
W The prostate gland undergoes many changes
during the course of a man's life. At birth, the
prostate is about the size of a pea. t grows only
slightly until puberty, when it begins to enlarge
rapidly, attaining normal adult size and shape,
about that of a walnut, when a man reaches his
early 20s. The gland generally remains stable
until about the mid-forties, when, in most men,
the prostate begins to enlarge again through a
process of cell multiplication. Hormonal changes
also occur in the prostate gland; testosterone
levels fall while dihydrotestosterone remain at
normal levels.
Pathophysiology Pathophysiology
1esLosLerone
ulhydrosLerone
8lnds Lo nuclear
Androgen
recepLors
Slgnals prosLaLe cells
Lo repllcaLe
LxacL cause of ldlopaLhlc
8lsk lacLors
Pyperplasla
ApopLosls
Male 30 y/o above
uleL eLhnlclLy
CbeslLy hormonal lx
uM 8ace
Smoklng lamlly Px
Alcohol use
Androgen
Slgnals growLh
facLors
esLrogen
8ecome senslLlve Lo growLh
SLlmulaLlng hormone
LaLe acLlvaLlon of
Cell growLh
3alpha
reducLase
1he paLhophyslology epldemlology and naLural hlsLory of benlgn
prosLaLlc hyperplasla (8P) are lncompleLely undersLood however Lhe
developmenL of rellable lnsLrumenLs Lo measure sympLom severlLy
prosLaLlc enlargemenL and bladder ouLleL obsLrucLlon has allowed
ma[or advances ln Lhelr elucldaLlon 1he developmenL of lower urlnary
LracL sympLoms (Lu1S) ln Lhe aglng male ls lnfluenced Lo some degree
by Lhe severlLy of bladder ouLleL obsLrucLlon and prosLaLlc enlargemenL
AlLhough Lhe developmenL of Lu1S bladder ouLleL obsLrucLlon and 8P
are agedependenL Lhey are noL necessarlly causally relaLed Lhere are
many oLher facLors lnvolved ln Lhe paLhophyslology of Lu1S 1he
cllnlcally lmporLanL parameLers of dlsease progresslon ln men wlLh
moderaLe Lo severe Lu1S and low peak flow raLes are sympLom
progresslon and Lhe developmenL of acuLe urlnary reLenLlon (Au8) 1he
rlsk of Au8 ls relaLed Lo boLh basellne serum prosLaLespeclflc anLlgen
level and prosLaLe volume ln men wlLh moderaLe prosLaLe enlargemenL
Lhe rlsk of Au8 appears Lo be hlgh enough Lo [usLlfy lnLervenLlon wlLh a
3reducLase lnhlblLor ln order Lo reduce Lhls rlsk
' ' aboratory and Diagnostic aboratory and Diagnostic
Test Test
W PSA TEST
W The purpose of the prostate-specific antigen (PSA) test,
along with the digital rectal examination, is to rule out
prostate cancer as the cause of your symptoms or to
raise warning signs that you need to be evaluated
further.
W The PSA test measures PSA levels in a man's blood.
Most men have low levels of PSA in the blood. Higher
than normal levels may indicate that prostate cancer is
present. However, about 25 percent to 30 percent of
men with elevated PSA levels have other reasons for
this result. Higher levels of PSA may be caused by BPH,
prostate inflammation, prostate infection, or even age
and hereditary factors.
W As a result, your doctor should discuss the PSA test with
you. f it is negative and you have a digital rectal
examination negative for prostate cancer, this is a
reassuring result and good evidence that you do not
have prostate cancer. You and your doctor can move on
to the best strategy for treating your BPH or other
diagnosed condition.
W However, if the PSA test is positive, it may or may not be
due to the presence of prostate cancer. You and your
doctor will need to follow through to be sure. Your doctor
may recommend repeating the PSA test to see if levels
climb higher, take a biopsy of your prostate tissue, or
perform other tests, including imaging tests of your
prostate.
W Because the PSA test registers a false positive
in a relatively high percentage of men, it's best
that you and your doctor are prepared for the
possibility of a positive test. Because the PSA
test can lead to more invasive testing (biopsy),
you and your doctor should discuss this
possibility. Some variations of the PSA test that
have been developed to make PSA results more
specific include the measurement of PSA
velocity (PSAV), free-total PSA ratio, complexed
PSA (cPSA), and PSA density (PSAD).
W &rine and BIood Testing
W ther laboratory tests that may be useful
for the doctor to order include a urinalysis
(diagnostic analysis of your urine) to rule
out the presence of an infection and blood
tests for signs of diabetes (which can also
cause nighttime urination), heart disease,
or other problems.
W &rinaIysis
W A urinalysis may be performed to detect signs of
bleeding or infection. A urinalysis involves a
physical and chemical examination of urine. n
addition, the urine is spun in a centrifuge to allow
sediments containing blood cells, bacteria, and
other particles to collect. This sediment is then
examined under a microscope. Although urinary
infection is uncommon in younger men, it occurs
more frequently in older men, particularly those
with BPH. A urinalysis also helps rule out bladder
cancer.
W B&
W This is an indicator of renal function and
perfusion, dietary intake of CH and the
level of protein metabolism.
W reatinine
W n men with symptoms, blood tests are
performed to measure a substance called
serum creatinine, which is a marker for
kidney trouble. Kidney problems exist in
an average of 13.6% of BPH patients.
Studies have reported rates as high as
30% and as low as 0.3%.
W ther aboratory Test
W f the results of the above tests suggest
you may have BPH, your health care
provider will probably want to perform
additional laboratory tests to confirm the
diagnosis and determine how severe your
condition is.
W &rine fIow test
W Measures the amount and strength of
urine flow. A rate of 15 milliliters per
second or greater is normal. A rate of 10
to 15 milliliters per second is associated
with mild to moderate symptoms. A rate of
less than 10 milliliters per second may
suggest moderate to severe BPH.
W Postvoid residue voIume test
W Ultrasound imaging to detect if you can
empty your bladder when you urinate.
W &Itrasound
W An imaging test of your prostate performed
by inserting a probe in your rectum to
determine the size of the prostate and to
detect any blockages or obstructions, such
as ones caused by a kidney stone,
prostate stone, or tumor.
W ytoscopy
W A cytoscope (a lighted probe) is placed
into your urethra to look for visible tissue
changes in your urethra and urinary
bladder
W &rodynamic studies
W This involves a series of tests in which a small catheter
is threaded through the urethra and into the bladder so
that bladder pressure and function can be measured.
Your doctor may want to perform this test if he or she
suspects your symptoms could be related to a bladder or
a neurologic problem.
W More extensive imaging of your bladder, urinary tract,
and kidneys may be appropriate if your doctor suspects
you have urinary tract or kidney damage, or other
disorders in addition to BPH. This is not generally
necessary if you have no other problems besides BPH
causing problems that have not advanced beyond
urinary symptoms
' ' SurgicaI management SurgicaI management
W MinimaIIy nvasive Therapy
W Because drug treatment is not effective in
all cases, researchers in recent years
have developed a number of procedures
that relieve BPH symptoms but are less
invasive than conventional surgery.
W TransurethraI microwave procedures
W n 1996, the FDA approved a device that uses microwaves to heat
and destroy excess prostate tissue. n the procedure called
transurethral microwave thermotherapy (TUMT), the device sends
computer-regulated microwaves through a catheter to heat selected
portions of the prostate to at least 111 degrees Fahrenheit. A
cooling system protects the urinary tract during the procedure.
W The procedure takes about 1 hour and can be performed on an
outpatient basis without general anesthesia. TUMT has not been
reported to lead to erectile dysfunction or incontinence.
W Although microwave therapy does not cure BPH, it reduces urinary
frequency, urgency, straining, and intermittent flow. t does not
correct the problem of incomplete emptying of the bladder. ngoing
research will determine any long-term effects of microwave therapy
and who might benefit most from this therapy.
W TransurethraI needIe abIation
W Also in 1996, the FDA approved the minimally
invasive transurethral needle ablation (TUA)
system for the treatment of BPH.
W The TUA system delivers low-level
radiofrequency energy through twin needles to
burn away a well-defined region of the enlarged
prostate. Shields protect the urethra from heat
damage. The TUA system improves urine flow
and relieves symptoms with fewer side effects
when compared with transurethral resection of
the prostate (TURP). o incontinence or
impotence has been observed.
W ater-induced thermotherapy
W This therapy uses heated water to destroy
excess tissue in the prostate. A catheter
containing multiple shafts is positioned in the
urethra so that a treatment balloon rests in the
middle of the prostate. A computer controls the
temperature of the water, which flows into the
balloon and heats the surrounding prostate
tissue. The system focuses the heat in a precise
region of the prostate. Surrounding tissues in the
urethra and bladder are protected. Destroyed
tissue either escapes with urine through the
urethra or is reabsorbed by the body.
W igh-intensity focused uItrasound
W The use of ultrasound waves to destroy
prostate tissue is still undergoing clinical
trials in the United States. The FDA has
not yet approved high-intensity focused
ultrasound.
W SurgicaI Treatment
W Most doctors recommend removal of the
enlarged part of the prostate as the best long-
term solution for patients with BPH. With surgery
for BPH, only the enlarged tissue that is pressing
against the urethra is removed; the rest of the
inside tissue and the outside capsule are left
intact. Surgery usually relieves the obstruction
and incomplete emptying caused by BPH. The
following section describes the types of surgery
that are used.
W TransurethraI surgery
W n this type of surgery, no external incision is needed.
After giving anesthesia, the surgeon reaches the
prostate by inserting an instrument through the urethra.
W A procedure called transurethral resection of the prostate
(TURP) is used for 90 percent of all prostate surgeries
done for BPH. With TURP, an instrument called a
resectoscope is inserted through the penis. The
resectoscope, which is about 12 inches long and 1/2
inch in diameter, contains a light, valves for controlling
irrigating fluid, and an electrical loop that cuts tissue and
seals blood vessels.
W During the 90-minute operation, the surgeon
uses the resectoscope's wire loop to remove the
obstructing tissue one piece at a time. The
pieces of tissue are carried by the fluid into the
bladder and then flushed out at the end of the
operation.
W Most doctors suggest using TURP whenever
possible. Transurethral procedures are less
traumatic than open forms of surgery and
require a shorter recovery period. ne possible
side effect of TURP is retrograde, or backward,
ejaculation. n this condition, semen flows
backward into the bladder during climax instead
of out the urethra.
W TransurethraI incision of the prostate (T&P)
W nstead of removing tissue, as with TURP, this
procedure widens the urethra by making a few
small cuts in the bladder neck, where the urethra
joins the bladder, and in the prostate gland itself.
Although some people believe that TUP gives
the same relief as TURP with less risk of side
effects such as retrograde ejaculation, its
advantages and long-term side effects have not
been clearly established.
W pen surgery
W n the few cases when a transurethral procedure cannot
be used, open surgery, which requires an external
incision, may be used. pen surgery is often done when
the gland is greatly enlarged, when there are
complicating factors, or when the bladder has been
damaged and needs to be repaired. The location of the
enlargement within the gland and the patient's general
health help the surgeon decide which of the three open
procedures to use.
W With all the open procedures, anesthesia is given and an
incision is made. nce the surgeon reaches the prostate
capsule, he or she scoops out the enlarged tissue from
inside the gland.
W Suprapubic prostatectomy
W Suprapubic prostatectomy (also called transvesical
prostatectomy) is a procedure to remove the prostatic
overgrowth via a different surgical route. The suprapubic
approach utilizes an incision of the lower anterior (front)
bladder wall. The primary advantage over the retropubic
approach is that the suprapubic route allows for direct
visualization of the bladder neck and bladder mucosa.
Because of this, the procedure is ideally suited for
persons who have bladder complications, as well as
obese men. The major disadvantage is that visualization
of the top part of the tumor is reduced. Additionally, with
the subrapubic approach, hemostasis (stoppage of
bleeding during surgery) may be more difficult due to
poor visualization after removal of the tumor.
W #etropubic prostatectomy
W The retropubic prostatectomy is
accomplished through a direct incision of
the anterior (front) prostatic capsule. The
overgrowth of glandular cells (hyperplastic
prostatic adenoma) is removed. These are
the cells forming a mass in the prostate
because of their abnormal multiplication.
W #adicaI PerineaI Prostatectomy
W The surgical incision is made in the space
between the anus and the scrotum. The
approach is particularly effective for patients who
have undergone previous abdominal surgery,
and have an extensive amount of surgical
adhesions in the area. The perineal approach
may not appropriate for those patients who are
massively obese. These contraindications may
be due to positioning, as patients need to be
placed in the exaggerated lithotomy position.
W aser surgery
W n March 1996, the FDA approved a surgical procedure
that employs side-firing laser fibers and d: YAG lasers
to vaporize obstructing prostate tissue. The doctor
passes the laser fiber through the urethra into the
prostate using a cystoscope and then delivers several
bursts of energy lasting 30 to 60 seconds. The laser
energy destroys prostate tissue and causes shrinkage.
As with TURP, laser surgery requires anesthesia and a
hospital stay. ne advantage of laser surgery over
TURP is that laser surgery causes little blood loss. Laser
surgery also allows for a quicker recovery time. But laser
surgery may not be effective on larger prostates. The
long-term effectiveness of laser surgery is not known.
W ewer procedures that use laser technology can be
performed on an outpatient basis.
W PhotoseIective vaporization of the
prostate (P'P)
W PVP uses a high-energy laser to destroy
prostate tissue and seal the treated area.
W nterstitiaI Iaser coaguIation
W Unlike other laser procedures, interstitial
laser coagulation places the tip of the
fiberoptic probe directly into the prostate
tissue to destroy it.
W P#STATE-SPE ATE
W Prostate-specific antigen (PSA)
W s a protein produced by the cells of the prostate
gland. PSA is present in small quantities in the
serum of men with healthy prostates, but is often
elevated in the presence of prostate cancer and
in other prostate disorders. A blood test to
measure PSA is considered the most effective
test currently available for the early detection of
prostate cancer, but this effectiveness has also
been questioned.
W Rising levels of PSA over time are associated
with both localized and metastatic prostate
cancer (CaP).
W Prostate-specific antigen (PSA), also known as
aIIirein , seminin, semenogeIase, y-
seminoprotein and P-30 antigen) is a 34 kD
glycoprotein manufactured almost exclusively by
the prostate gland; PSA is produced for the
ejaculate where it liquifies the semen in the
seminal coagulum and allows sperm to swim
freely. t is also believed to be instrumental in
dissolving the cervical mucous cap, allowing the
entry of sperm.
W t is a serine protease (EC 3.4.21.77) enzyme,
the gene of which is located on the nineteenth
chromosome (19q13).
Serum PSA
W PSA is normally present in the blood at very low levels.
The reference range of less than 4 ng/mL for the first
commercial PSA test, the Hybritech Tandem-R PSA test
released in February 1986, was based on a study that
found 99% of 472 apparently healthy men had a total
PSA level below 4 ng/mLthe upper limit of normal is
much less than 4 ng/mL. ncreased levels of PSA may
suggest the presence of prostate cancer. However,
prostate cancer can also be present in the complete
absence of an elevated PSA level, in which case the test
result would be a false negative. besity has been
reported to reduce serum PSA levels. Delayed early
detection may partially explain worse outcomes in obese
men with early prostate cancer.
W PSA levels can be also increased by
prostate infection, irritation, benign
prostatic hyperplasia (BPH), and recent
ejaculation, producing a false positive
result. Digital rectal examination (DRE)
has been shown in several studies to
produce an increase in PSA. However, the
effect is clinically insignificant, since DRE
causes the most substantial increases in
patients with PSA levels already elevated
over 4.0 ng/mL.
W Most PSA in the blood is bound to serum
proteins. A small amount is not protein bound
and is called free PSA. n men with prostate
cancer the ratio of free (unbound) PSA to total
PSA is decreased. The risk of cancer increases
if the free to total ratio is less than 25%. (See
graph at right.) The lower the ratio the greater
the probability of prostate cancer. Measuring the
ratio of free to total PSA appears to be
particularly promising for eliminating
unnecessary biopsies in men with PSA levels
between 4 and 10 ng/mL. However, both total
and free PSA increase immediately after
ejaculation, returning slowly to baseline levels
within 24 hours.
PSTPE#AT'E A#E PSTPE#AT'E A#E
W ontinuous BIadder rrigation
W Continuous bladder irrigation is a medical
procedure which is usually performed for
one of two reasons. First, it is performed to
minimize the chances of blood clots
forming in the bladder following certain
types of surgery. Second, it is a means of
injecting medication into the bladder to
fight an infection or for some other reason.
W Continuous bladder irrigation is not a terribly
complicated procedure, though specialized
instruments are used. The procedure does have
to be monitored fairly closely however to ensure
that the desired results are being obtained, and
also to ensure no complications arise. The
procedure may become necessary when there is
either a disease of the bladder, or the function of
the bladder is being impaired by another body
condition, such as an enlarged prostrate gland.
W The Procedure
W The continuous bladder irrigation procedure is usually
ordered by a physician and then performed either by the
physician, a registered nurse, or a nurse practitioner. A
special catheter is inserted through the urethra into the
bladder. nce inserted, a small balloon filled with a
saline solution helps keep it in place. Both irrigation and
urination occur through the catheter. The catheter is
retained until either the proper amount of medication has
been administered, or if there has been surgery
performed, until the urine is essentially free of
blood. Following certain types of surgery the catheter
may have to remain in place several days, but 24 hours
is more common.
' ' ommon ursing ommon ursing
Diagnosis Diagnosis
W &rinary retention reIated to bIocage from enIarge
prostate gIand
W &rinary incontinence reIated to over distention of the
bIadder
W Disturbed sIeep pattern reIated to urinary urgency,
nocturia
W #is for infection reIated to inadequate primary
defences (stasis of urine)
W PotentiaI for renaI insufficiency
W mpaired urinary eIimination reIated to increase
urethraI occIusion
W Activity intoIerance reIated to body maIaise
W SIeep pattern disturbance reIated to urinary
incontinence
W #is for infection reIated to periodic
catheterization
W neffective therapeutic regimen reIated to
Iac of understanding of disease,
manifestation of medicaI treatment
W Acute pain reIated to bIadder spasm,
obstruction, surgicaI process
W Anxiety reIated to concerns over Ioss of
sexuaI functioning foIIowing prostate
surgery
W #is for injury(bIeeding) reIated to surgicaI
intervention
' ' Discharge (nstruction) Discharge (nstruction)
W M- nstructed the patient to continue medication
as ordered
W E- nstructed the patient to do exercise as
tolerated such as walking
W T- nstructed the patient to continue the
medication
W - 1. Encouraged patient to increase fluid intake
W 2. Encouraged patient to eat foods rich in
Vitamin C and utritious foods
W 3. Encourage patient to avoid salty and
fatty foods
W 4. Encourage patient to have enough
rest
W - nstructed to come back for follow-up
check-up
W D- Advised the patient to a diet as
tolerated but preferably avoiding salty and
fatty foods.