You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Cara Penyimpanan ObatDocument2 pagesCara Penyimpanan ObatLhian NieezNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Awareness of Diabetic Retinopathy Among Saudis With Diabetes Type 2 in Riyadh CityDocument5 pagesAwareness of Diabetic Retinopathy Among Saudis With Diabetes Type 2 in Riyadh CityFatty MaulidiraNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- t2dm Class Comparions ChartDocument1 paget2dm Class Comparions Chartpinkup1199No ratings yet
- Insulin Therapy in Critically IllDocument2 pagesInsulin Therapy in Critically IllNisbet SamuelNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Case Study t2d Management PDFDocument9 pagesCase Study t2d Management PDFpcxwaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Paula Mcclusky Aprn PresentationDocument18 pagesPaula Mcclusky Aprn Presentationapi-676449505No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Blood Glucose Units Conversion Table: Endocrinology & Diabetes UnitDocument1 pageBlood Glucose Units Conversion Table: Endocrinology & Diabetes UnitDrFarah Emad AliNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Essential Nutrients and Therapeutic Diets for Health and WellnessDocument12 pagesEssential Nutrients and Therapeutic Diets for Health and WellnesszabedahibrahimNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 12 30 11 AADE Insulin WhitePaper PrintDocument17 pages12 30 11 AADE Insulin WhitePaper PrintMiguel Angel Fonseca RiveraNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Module 8 Assessment and Management of Patients With DiabetesDocument44 pagesModule 8 Assessment and Management of Patients With DiabetesBlessed GarcianoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- About DapagliflozinDocument6 pagesAbout DapagliflozinUjjval GandhiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Type 2 Diabetes in Children and AdolescentsDocument16 pagesType 2 Diabetes in Children and AdolescentsCarlita Cari CclNo ratings yet
- Australian Diabetes Society Guidelines For Routine Glucose Control in HospitalDocument70 pagesAustralian Diabetes Society Guidelines For Routine Glucose Control in HospitalYovan PrakosaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Patient HbA1c level indicates diabetesDocument1 pagePatient HbA1c level indicates diabetesMajid MustafaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Accu Chek Performa System ManualDocument196 pagesAccu Chek Performa System ManualAhmedJumanNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- DIPSI GuidelinesDocument7 pagesDIPSI GuidelinesvinaypharmNo ratings yet
- EXPOSITORY ESSAY DiabetesDocument1 pageEXPOSITORY ESSAY DiabetesSaida BallesteroNo ratings yet
- MnhwejcihdfjcnfekcnDocument8 pagesMnhwejcihdfjcnfekcnDr IslamNo ratings yet
- JOURNAL CLUB Presentation: Presented by Phatcharaporn Dangtongdee 583150152-4 Section 3Document21 pagesJOURNAL CLUB Presentation: Presented by Phatcharaporn Dangtongdee 583150152-4 Section 3Phatcharaporn DangtongdeeNo ratings yet
- Mcqs On Diabetes Mellitus Update: FPSC No: 77 Submission DEADLINE: 19 March 2019, 12 NOONDocument3 pagesMcqs On Diabetes Mellitus Update: FPSC No: 77 Submission DEADLINE: 19 March 2019, 12 NOONAbdullah Zawary100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Kadar Glukosa Darah Sewaktu Pada Pasien Diabetes Melitus Tipe 2 Di Puskesmas Bahu Kota ManadoDocument9 pagesKadar Glukosa Darah Sewaktu Pada Pasien Diabetes Melitus Tipe 2 Di Puskesmas Bahu Kota ManadoMuhammad HasanNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Geriatric EndocrinologyDocument65 pagesGeriatric EndocrinologyZaidanNo ratings yet
- Blood Sugar Insulin Polyuria Polydipsia PolyphagiaDocument7 pagesBlood Sugar Insulin Polyuria Polydipsia PolyphagiankirrNo ratings yet
- Blood Glucose MonitoringDocument20 pagesBlood Glucose Monitoringask1400100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Jurnal 14.042 Teta Dea Kurnia Kusuma WardhaniDocument13 pagesJurnal 14.042 Teta Dea Kurnia Kusuma WardhaniTeta Dea KkwNo ratings yet
- 7 OAD DR - Elly 2015Document52 pages7 OAD DR - Elly 2015ainNo ratings yet
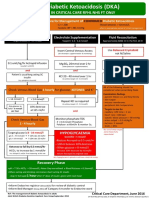
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocument1 pageAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Cares Assistance in Developing Independent Treatment of Type 2 Diabetes Mellitus Patients in Mantuil Village, Banjarmasin Selatan DistrictDocument5 pagesCares Assistance in Developing Independent Treatment of Type 2 Diabetes Mellitus Patients in Mantuil Village, Banjarmasin Selatan DistrictCANDRA KUSUMANEGARANo ratings yet
- Glycemic Control PDFDocument26 pagesGlycemic Control PDFangiolikkiaNo ratings yet
- Glycemic Variability in Type 2 Diabetes Patients with Chronic Kidney DiseaseDocument3 pagesGlycemic Variability in Type 2 Diabetes Patients with Chronic Kidney DiseaseSasi SekharNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)