You might also like
- AnesthesiaDocument18 pagesAnesthesiaZakria Al-HadadNo ratings yet
- Efusi Pleura PPT - Id.en (Repaired)Document17 pagesEfusi Pleura PPT - Id.en (Repaired)fitriaNo ratings yet
- Komplikasi CabutDocument4 pagesKomplikasi CabutivyNo ratings yet
- Postoperative Care in Functional Endoscopic: Sinus Surgery?Document4 pagesPostoperative Care in Functional Endoscopic: Sinus Surgery?Ida KatarinaNo ratings yet
- Local Anesthetic Systemic ToxicityDocument1 pageLocal Anesthetic Systemic Toxicitylaurad.benavidesNo ratings yet
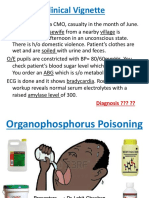
- Topic Review IntoxicationsDocument75 pagesTopic Review Intoxicationsdani_zurita_1No ratings yet
- 9384 - Original ResearchDocument3 pages9384 - Original ResearchAnita PrastiwiNo ratings yet
- 16 Bier BlockDocument28 pages16 Bier BlockJessica CNo ratings yet
- Articaine in Oral SurgeryDocument19 pagesArticaine in Oral SurgeryAimeeNo ratings yet
- MFD OSCE Sample Papers With Link To Full VersionDocument14 pagesMFD OSCE Sample Papers With Link To Full VersiongarimaNo ratings yet
- Drug Allergy BookDocument332 pagesDrug Allergy Bookmegah_asia13No ratings yet
- Principles of Periodontal SurgryDocument106 pagesPrinciples of Periodontal SurgrynusreenNo ratings yet
- Local Anesthesia in Pediatric DentistryDocument70 pagesLocal Anesthesia in Pediatric DentistryNicky Romeo100% (1)
- Ent Solved Kmu Seqs by RMC StudentsDocument68 pagesEnt Solved Kmu Seqs by RMC StudentsAamir Khan100% (1)
- Steroid in EntDocument113 pagesSteroid in Entdrazmy2006100% (1)
- Bagaimana Menangani Infeksi OdontogenikDocument37 pagesBagaimana Menangani Infeksi OdontogenikTiara IkaNo ratings yet
- Local Anesthetics: Richard D. Minshall, PHD Tobias Piegeler, MDDocument40 pagesLocal Anesthetics: Richard D. Minshall, PHD Tobias Piegeler, MDJohnBedaLatawanMalecdanNo ratings yet
- 6324-Article Text-21760-1-10-20210620Document3 pages6324-Article Text-21760-1-10-20210620Fritzienico BaskoroNo ratings yet
- Universitas Indonesia: U. Weber, M. Krammel, S. Linke, T. Hamp, T. Stimpfl, B. Reiter, W. PlӧchlDocument8 pagesUniversitas Indonesia: U. Weber, M. Krammel, S. Linke, T. Hamp, T. Stimpfl, B. Reiter, W. PlӧchlgoldenNo ratings yet
- Is Topical Photodynamic Therapy With 5-ALA, Using Tsai's Protocol, Useful in The Healing of Oral Potentially Malignant Disorders? A Systematic Review of The LiteratureDocument7 pagesIs Topical Photodynamic Therapy With 5-ALA, Using Tsai's Protocol, Useful in The Healing of Oral Potentially Malignant Disorders? A Systematic Review of The LiteratureBagis Emre GulNo ratings yet
- Suspected Anaphylactic Reactions Associated With AnaesthesiaDocument24 pagesSuspected Anaphylactic Reactions Associated With AnaesthesiaSayed AhmedNo ratings yet
- Darunday NCP Rot 3Document12 pagesDarunday NCP Rot 3Ezra Miguel DarundayNo ratings yet
- Local AnestheticsDocument7 pagesLocal AnestheticsEmmanuel CarrilloNo ratings yet
- Opfinalppt 160117042516 PDFDocument83 pagesOpfinalppt 160117042516 PDFV RakeshreddyNo ratings yet
- Dental Insethesiea Part 1Document45 pagesDental Insethesiea Part 1hasibNo ratings yet
- Handbook of Splinting and CastingDocument318 pagesHandbook of Splinting and Castingguillermina paz100% (1)
- Stolovitzky Et Al 2021 Effect of Radiofrequency Neurolysis On The Symptoms of Chronic Rhinitis A Randomized ControlledDocument7 pagesStolovitzky Et Al 2021 Effect of Radiofrequency Neurolysis On The Symptoms of Chronic Rhinitis A Randomized ControlledfrischaNo ratings yet
- Chronic Disease Management for Small AnimalsFrom EverandChronic Disease Management for Small AnimalsW. Dunbar GramNo ratings yet
- Genta Transtimpanica 4Document8 pagesGenta Transtimpanica 4natalia.gallinoNo ratings yet
- Local Anesthesia - Solution To Pain An OverviewDocument12 pagesLocal Anesthesia - Solution To Pain An OverviewG.S. Imanto UchihaNo ratings yet
- Complex Care Clinical Concept Map Sara Ciletti Youngstown State UniversityDocument9 pagesComplex Care Clinical Concept Map Sara Ciletti Youngstown State Universityapi-590353096No ratings yet
- Local Analgesia10.5.11Document14 pagesLocal Analgesia10.5.11Rakan KhtoomNo ratings yet
- Point of CareDocument5 pagesPoint of CareDaniela RochaNo ratings yet
- Masrial - Materi Kebijakan, Standar Dan Prosedur Aseptis Dispensing 270622-2Document59 pagesMasrial - Materi Kebijakan, Standar Dan Prosedur Aseptis Dispensing 270622-2EmaNo ratings yet
- Lateral Internal Sphincterotomy For Fissure-In-Ano RevisitedDocument6 pagesLateral Internal Sphincterotomy For Fissure-In-Ano RevisiteddoctortareqNo ratings yet
- Rot 3 - Darunday SicDocument9 pagesRot 3 - Darunday SicEzra Miguel DarundayNo ratings yet
- Invasive Sino-Aspergillosis in ImmunocompetentDocument5 pagesInvasive Sino-Aspergillosis in Immunocompetentabeer alrofaeyNo ratings yet
- S5 Rehani Introduction of The TopicDocument64 pagesS5 Rehani Introduction of The TopicIvánHernándezNo ratings yet
- Darier-White Disease: A Rare Genetic DisorderDocument4 pagesDarier-White Disease: A Rare Genetic Disorderanis utamiNo ratings yet
- A Quazi-Experimental Study To Compare Outcome Between Lateral Sphincterotomy, Topical 2% Diltiazem and Topical 0.2% Nitro-Glycerine in The Management of Chronic Anal FissureDocument4 pagesA Quazi-Experimental Study To Compare Outcome Between Lateral Sphincterotomy, Topical 2% Diltiazem and Topical 0.2% Nitro-Glycerine in The Management of Chronic Anal FissureIjsrnet EditorialNo ratings yet
- Lfurbot,+journal+manager,+aabp 2018 v52 2 004 CaseSeriesSurgicalTreatmentDocument9 pagesLfurbot,+journal+manager,+aabp 2018 v52 2 004 CaseSeriesSurgicalTreatmentPediatrics Department OPD CRMCNo ratings yet
- Anaphylaxis Update: Be Prepared!: Ari R Cohen, MD, FAAP Massachusetts General Hospital Boston, MADocument45 pagesAnaphylaxis Update: Be Prepared!: Ari R Cohen, MD, FAAP Massachusetts General Hospital Boston, MAAsfiksia NeonatorumNo ratings yet
- Ed 58Document8 pagesEd 58Luís CorreiaNo ratings yet
- Managing Complications in Glaucoma SurgeryDocument121 pagesManaging Complications in Glaucoma Surgeryshetya_8212No ratings yet
- Anaesthetic AwarenessDocument21 pagesAnaesthetic AwarenessPeter KamNo ratings yet
- Ijced 3 (3) 101-109Document9 pagesIjced 3 (3) 101-109GembongSatriaMahardhikaNo ratings yet
- Anestesi LokalDocument12 pagesAnestesi LokalKurniatiKhasanahQhafisaQurratul'ainNo ratings yet
- Hyperuricemia and Gout - A New Treatment OptionDocument39 pagesHyperuricemia and Gout - A New Treatment OptionDinda YusditiraNo ratings yet
- Low-Fluence 1,064-nm Laser Hair Reduction For Pseudofolliculitis Barbae in Skin Types IV, V, and VIDocument10 pagesLow-Fluence 1,064-nm Laser Hair Reduction For Pseudofolliculitis Barbae in Skin Types IV, V, and VIRada TrifonovNo ratings yet
- Successful Treatment of Lipoatrophy With Normal Saline 1Document3 pagesSuccessful Treatment of Lipoatrophy With Normal Saline 1Atena KhrdmndNo ratings yet
- Lary 23467Document8 pagesLary 23467Dwi juliana DewiNo ratings yet
- JMBS2010 (1 8)Document5 pagesJMBS2010 (1 8)DoVa XuNo ratings yet
- Dihematoporphyrin Ether-Induced Photosensitivity in Laryngeal Papilloma PatientsDocument8 pagesDihematoporphyrin Ether-Induced Photosensitivity in Laryngeal Papilloma PatientsDayse CSMNo ratings yet
- KSPAN Recognition and Treatment of Local Anesthetic Systemic ToxicityDocument39 pagesKSPAN Recognition and Treatment of Local Anesthetic Systemic ToxicityAli AftabNo ratings yet
- Incidence of Complications of Inferior Alveolar Nrve BlockDocument6 pagesIncidence of Complications of Inferior Alveolar Nrve Blockmatias112No ratings yet
- Articaine and ParasthesiaDocument2 pagesArticaine and ParasthesiaDentalLearningNo ratings yet
- Open Comparative Study of Efficacy and Safety of Ketoconazole Soap and Oral Ketoconazole in Tinea VersicolorDocument5 pagesOpen Comparative Study of Efficacy and Safety of Ketoconazole Soap and Oral Ketoconazole in Tinea VersicolorYohanes WidjajaNo ratings yet
- Cytopathology of the Head and Neck: Ultrasound Guided FNACFrom EverandCytopathology of the Head and Neck: Ultrasound Guided FNACNo ratings yet
- Passive Aggressive Communication StyleDocument18 pagesPassive Aggressive Communication StyleSonu RjNo ratings yet
- Aerobic Gymnastics Information GuideDocument6 pagesAerobic Gymnastics Information GuideАлёна ГлушковаNo ratings yet
- Policies and Guidelines Related To HivDocument50 pagesPolicies and Guidelines Related To HivGandimarei100% (1)
- ScheduleDocument1 pageSchedule3E, KENNADY KARUNAKARAN, PRINCENo ratings yet
- Cosmetic Uses of Activated CharcoalDocument3 pagesCosmetic Uses of Activated CharcoalTrần Duy TânNo ratings yet
- Fat To Fabulous PDFDocument197 pagesFat To Fabulous PDFjjleejustina100% (1)
- Special UCF Grease 605Document5 pagesSpecial UCF Grease 605MichaelNo ratings yet
- Reiki: Center For Integrative MedicineDocument2 pagesReiki: Center For Integrative MedicineangelineibibNo ratings yet
- A Framework For Practice With High Risk Young People 12 17 YrsDocument16 pagesA Framework For Practice With High Risk Young People 12 17 YrselaineNo ratings yet
- Research - Group Echo Edited SurveyDocument29 pagesResearch - Group Echo Edited SurveyMONFORTE TRIXIE BALAGOSANo ratings yet
- Visual Impairments in Young Children: Fundamentals of and Strategies For Enhancing DevelopmentDocument13 pagesVisual Impairments in Young Children: Fundamentals of and Strategies For Enhancing Developmentfadil ahmadiNo ratings yet
- 4.3 FA2.A MCQ Management Theories Planning - NCM 119 NURSING LEADERSHIP AND MANAGEMENTDocument10 pages4.3 FA2.A MCQ Management Theories Planning - NCM 119 NURSING LEADERSHIP AND MANAGEMENTGil GanibanNo ratings yet
- Upper/lower 2 Day SplitDocument2 pagesUpper/lower 2 Day SplitSebas JepNo ratings yet
- Patient Details Specimen Details Physician DetailsDocument1 pagePatient Details Specimen Details Physician DetailsMax WellsNo ratings yet
- Infographics in Anesthesiology: Complex Information For Anesthesiologists Presented Quickly and ClearlyDocument1 pageInfographics in Anesthesiology: Complex Information For Anesthesiologists Presented Quickly and ClearlyParvathy R NairNo ratings yet
- Persistent Pursuit of Need-Satisfying Goals Leads To Increased Happiness: A 6-Month Experimental Longitudinal StudyDocument10 pagesPersistent Pursuit of Need-Satisfying Goals Leads To Increased Happiness: A 6-Month Experimental Longitudinal StudyruxandaNo ratings yet
- Case Study Drinking Up The PaycheckDocument1 pageCase Study Drinking Up The Paychecksmart.soldier110No ratings yet
- Mango PhytochemicalsDocument21 pagesMango PhytochemicalsMaria Elena MaldonadoNo ratings yet
- MisofemDocument2 pagesMisofemAyoade Rokeeb AyomideNo ratings yet
- ICU Investigation SheetDocument2 pagesICU Investigation SheetAnand VijayNo ratings yet
- G.R. No. 226907, July 22, 2019 Third Division Peralta, JDocument2 pagesG.R. No. 226907, July 22, 2019 Third Division Peralta, Jshookt panboiNo ratings yet
- Lab Man Prelims To FinalsDocument42 pagesLab Man Prelims To FinalsMica CapistranoNo ratings yet
- Emergency Trolley GuidelineDocument3 pagesEmergency Trolley GuidelineNur SusiawantyNo ratings yet
- Pneumonia in ChildrenDocument4 pagesPneumonia in ChildrenkuterinbatNo ratings yet
- AbortionDocument38 pagesAbortionSunny P JNo ratings yet
- Ra 8371Document32 pagesRa 8371Jesh RadazaNo ratings yet
- Detailed Lesson Plan EPP6 TLEIE6-0b-3Document9 pagesDetailed Lesson Plan EPP6 TLEIE6-0b-3Torres, Emery D.100% (1)
- CMS Has Updated This Memorandum To Be Consistent With More Recently Issued MemosDocument11 pagesCMS Has Updated This Memorandum To Be Consistent With More Recently Issued Memosflojanas3858No ratings yet
- Postpartum Care PlanDocument6 pagesPostpartum Care Planallie-jones-6489100% (27)
- OHS - U-5 - Health Screening MeasuresDocument42 pagesOHS - U-5 - Health Screening Measuressidda lingeshaNo ratings yet