You might also like
- Cataract: The Role of Nurses in Diagnosis, Surgery and AftercareDocument5 pagesCataract: The Role of Nurses in Diagnosis, Surgery and AftercareFara Sakina RahmaNo ratings yet
- Biometry: Dr. Sanjay Kumar SarkerDocument67 pagesBiometry: Dr. Sanjay Kumar SarkerNiloy Basak100% (3)
- Osce OftalmologíaDocument232 pagesOsce OftalmologíaJavierNo ratings yet
- OphthoBook 1-6.0Document180 pagesOphthoBook 1-6.0David Cheng100% (1)
- Penetrating Keratoplasty StepsDocument57 pagesPenetrating Keratoplasty StepsVishwajeetNo ratings yet
- Tugas Baca RS IndraDocument28 pagesTugas Baca RS IndraMade Surya DinajayaNo ratings yet
- Referat SMILEDocument10 pagesReferat SMILEarumNo ratings yet
- New Technique of Deep Anterior Lamellar KeratoplastyDocument5 pagesNew Technique of Deep Anterior Lamellar KeratoplastyLeonardo TorquettiNo ratings yet
- Management of Post-Keratoplasty AstigmatismDocument11 pagesManagement of Post-Keratoplasty Astigmatismdianis0506No ratings yet
- Minimal Duration Cataract Surgery (MDCS) - Small Incision Cataract Surgery (SICS) Without Superior Rectus Stitch, No Conjunctival Flap and No CauterizationDocument4 pagesMinimal Duration Cataract Surgery (MDCS) - Small Incision Cataract Surgery (SICS) Without Superior Rectus Stitch, No Conjunctival Flap and No CauterizationBayu PrakosoNo ratings yet
- Surgical Technique Tips and PearlsDocument6 pagesSurgical Technique Tips and Pearls7zhm9d9dbpNo ratings yet
- Post-Keratoplasty Astigmatism Management by RelaxiDocument7 pagesPost-Keratoplasty Astigmatism Management by Relaximedamif3No ratings yet
- Moderator - DR Prof. R.K. Bundela Presented by - Dr. Mohd Raza .Document44 pagesModerator - DR Prof. R.K. Bundela Presented by - Dr. Mohd Raza .alpana100% (1)
- Cataract Coach BookDocument62 pagesCataract Coach Bookravian8bNo ratings yet
- Flap Thickness and The Risk of ComplicationsDocument20 pagesFlap Thickness and The Risk of ComplicationsDarwin VasquezNo ratings yet
- Lasik Chapter 22Document13 pagesLasik Chapter 22christine nathalia loupattyNo ratings yet
- Mecegah Komplikasi SicsDocument9 pagesMecegah Komplikasi Sicsinna_luv_u9006No ratings yet
- Pi Is 1319453411000580Document5 pagesPi Is 1319453411000580Hario Tri HendrokoNo ratings yet
- Dada 2007Document4 pagesDada 2007asfwegereNo ratings yet
- Properties and Advantages: Intracorneal Ring Segments - Review of The Literature. Eye & Contact Lens 2014 40:365-370Document7 pagesProperties and Advantages: Intracorneal Ring Segments - Review of The Literature. Eye & Contact Lens 2014 40:365-370Ahmed AYASHNo ratings yet
- Endothelial KeratoplastyDocument6 pagesEndothelial KeratoplastyRijal SaputroNo ratings yet
- 05 EcceDocument9 pages05 EccebebibebihoNo ratings yet
- PhacoemulsificationDocument54 pagesPhacoemulsificationIshita Kinra100% (1)
- Are Intrastromal Treatments The Future of Refractive Surgery?Document11 pagesAre Intrastromal Treatments The Future of Refractive Surgery?lacisag100% (1)
- DcsDocument4 pagesDcsdisk_la_podu100% (1)
- Cataract Surgery: Past-Present-FutureDocument44 pagesCataract Surgery: Past-Present-FutureNica Lopez FernandezNo ratings yet
- 06 Small Incision Cataract SurgeryDocument21 pages06 Small Incision Cataract SurgeryApriliani SanitiNo ratings yet
- A To Z of Relex Smile: All You Need To Know: Review ArticleDocument7 pagesA To Z of Relex Smile: All You Need To Know: Review ArticleStefanNo ratings yet
- Management of Astigmatism in Conjunction With Clear Corneal Phaco SurgeryDocument12 pagesManagement of Astigmatism in Conjunction With Clear Corneal Phaco SurgeryRIe HAnaNo ratings yet
- Keratoplasty XDocument41 pagesKeratoplasty XArunimaNo ratings yet
- Descemet Membrane Endothelial Keratoplasty in Pseudophakic Bullous Keratopathy: Outcomes and Evidence-Based SuggestionsDocument6 pagesDescemet Membrane Endothelial Keratoplasty in Pseudophakic Bullous Keratopathy: Outcomes and Evidence-Based SuggestionsRaymond 102014223No ratings yet
- Ormond 2013Document12 pagesOrmond 2013Hafiz AlfarizieNo ratings yet
- Surgical Management of Senile CataractDocument39 pagesSurgical Management of Senile CataractKarthik ChellaNo ratings yet
- Pershing 2011Document6 pagesPershing 2011asfwegereNo ratings yet
- Zepto-Rhexis IndianJOphthalmol 2018Document4 pagesZepto-Rhexis IndianJOphthalmol 2018dwongNo ratings yet
- Femtosecond Laser Cataract Surgery: Sepehr Feizi, MDDocument1 pageFemtosecond Laser Cataract Surgery: Sepehr Feizi, MDHario Tri HendrokoNo ratings yet
- Keratoplasty: By: Esmaeil Hashemi MC: 410a Dept. of OphthalmologyDocument43 pagesKeratoplasty: By: Esmaeil Hashemi MC: 410a Dept. of OphthalmologyEsmaeil HashemiNo ratings yet
- Phacoemulsification Versus Extracapsular Cataract Extraction: Where Do We Stand?Document6 pagesPhacoemulsification Versus Extracapsular Cataract Extraction: Where Do We Stand?Vlady BordaNo ratings yet
- Small Incision Cataract SurgeryDocument8 pagesSmall Incision Cataract Surgerykefi998100% (3)
- Retinal Physician - Visualization in Vitrectomy - An UpdateDocument12 pagesRetinal Physician - Visualization in Vitrectomy - An UpdateDr. M. Hannan JamilNo ratings yet
- Modified Sewing Machine Technique For IridodialysiDocument8 pagesModified Sewing Machine Technique For IridodialysiRonal PerinoNo ratings yet
- ReLExCourseHandout IC80 Reinstein - 2013Document13 pagesReLExCourseHandout IC80 Reinstein - 2013David MartínezNo ratings yet
- Scleral Fixation and PKDocument4 pagesScleral Fixation and PKPatricia ChirinosNo ratings yet
- AR Refractive Surgery-KalkidanDocument47 pagesAR Refractive Surgery-Kalkidanhenok birukNo ratings yet
- Vitrectomy Surgery For Primary Retinal DetachmentDocument8 pagesVitrectomy Surgery For Primary Retinal DetachmentAvluz AdiansuhNo ratings yet
- Senile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsDocument5 pagesSenile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsAhmad FahroziNo ratings yet
- Review Article Review of Manual Small Incision Cataract SurgeryDocument8 pagesReview Article Review of Manual Small Incision Cataract SurgeryFadhila AnggariniNo ratings yet
- Lasik Technology Review in MalaysiaDocument20 pagesLasik Technology Review in Malaysiakey3hseNo ratings yet
- Combined Double-Needle Flanged-Haptic Intrascleral Fixation of An Intraocular Lens and Descemet-Stripping Endothelial KeratoplastyDocument7 pagesCombined Double-Needle Flanged-Haptic Intrascleral Fixation of An Intraocular Lens and Descemet-Stripping Endothelial Keratoplastyintan juitaNo ratings yet
- Pterygium Management - Today: Medical ScienceDocument3 pagesPterygium Management - Today: Medical ScienceLiestiono NasiNo ratings yet
- Dwdudfw: Sangeeta Abrol MS, Neeraj Varma MSDocument4 pagesDwdudfw: Sangeeta Abrol MS, Neeraj Varma MSnikhil mahajanNo ratings yet
- Corneal TransplantationDocument10 pagesCorneal TransplantationKabelo MaruvaNo ratings yet
- Cataract Surgery in Corneal Transplantation: ReviewDocument5 pagesCataract Surgery in Corneal Transplantation: ReviewMariana Luzardo bravoNo ratings yet
- 0210 f8 DanasouryDocument4 pages0210 f8 DanasouryLJANo ratings yet
- Cryotherapy For Ocular Tumors-New Finger-Tip' Cryoprobes Provide A Wide Range of Uses and ApplicationsDocument2 pagesCryotherapy For Ocular Tumors-New Finger-Tip' Cryoprobes Provide A Wide Range of Uses and ApplicationsGusti Zidni FahmiNo ratings yet
- Flap Konjungtiva SusanDocument10 pagesFlap Konjungtiva SusanGlaucoma UnhasNo ratings yet
- Graft Selection: Full-Thickness Skin GraftDocument8 pagesGraft Selection: Full-Thickness Skin GraftIkhsanNo ratings yet
- (123doc) Opthalmic Microsurgical Suturing Techniques Part 9Document15 pages(123doc) Opthalmic Microsurgical Suturing Techniques Part 9TEODORA MIHAELA PELEASANo ratings yet
- Cohen - 5 - Preparation For Treament - Tooth IsolationDocument15 pagesCohen - 5 - Preparation For Treament - Tooth IsolationMufidah NurulNo ratings yet
- An Introduction To Corneal TransplantationDocument2 pagesAn Introduction To Corneal TransplantationNovii NoviiNo ratings yet
- The History of Corneal Transplantation: Chad K RostronDocument14 pagesThe History of Corneal Transplantation: Chad K RostronDebby SiltamiNo ratings yet
- Textbook of Refractive Laser Assisted Cataract Surgery (ReLACS)From EverandTextbook of Refractive Laser Assisted Cataract Surgery (ReLACS)No ratings yet
- Practical Handbook for Small-Gauge Vitrectomy: A Step-By-Step Introduction to Surgical TechniquesFrom EverandPractical Handbook for Small-Gauge Vitrectomy: A Step-By-Step Introduction to Surgical TechniquesNo ratings yet
- Cosmetic Contact Lens-Related Corneal Infections in AsiaDocument8 pagesCosmetic Contact Lens-Related Corneal Infections in AsiaAnggitaNo ratings yet
- Willcox 2017Document38 pagesWillcox 2017Anggia BungaNo ratings yet
- Chapter 1 Origins of The Contact Lens PDFDocument19 pagesChapter 1 Origins of The Contact Lens PDFfakenameNo ratings yet
- Ebook Ocular Pathology PDF Full Chapter PDFDocument67 pagesEbook Ocular Pathology PDF Full Chapter PDFshannon.boersma620100% (25)
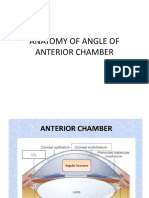
- Anatomy of Angle of Anterior ChamberDocument67 pagesAnatomy of Angle of Anterior ChamberRahnaNo ratings yet
- Healthy Eyes - 11 March 2018Document8 pagesHealthy Eyes - 11 March 2018Irfan AksariNo ratings yet
- MPSC Exams of Opthalmology 2Document7 pagesMPSC Exams of Opthalmology 2Hussein AliNo ratings yet
- Escalas de EfronDocument2 pagesEscalas de Efronkarina100% (1)
- MYDRIATICDocument6 pagesMYDRIATICManik BashaNo ratings yet
- Lecture 3 Soft Contact DesignsDocument58 pagesLecture 3 Soft Contact DesignswillemlrouxNo ratings yet
- Lens & Cataract Review NN - ppt2Document113 pagesLens & Cataract Review NN - ppt2Yonas AbrahamNo ratings yet
- Latest Current Affairs-2013 (Till July 2013)Document167 pagesLatest Current Affairs-2013 (Till July 2013)kanabaramitNo ratings yet
- Cataract Surgery in Patients With Corneal Opacities: Researcharticle Open AccessDocument10 pagesCataract Surgery in Patients With Corneal Opacities: Researcharticle Open AccesszulmiyettyNo ratings yet
- Review On The Myopia PandemicDocument8 pagesReview On The Myopia PandemicIlona HiariejNo ratings yet
- Biology Investigatory ProjectDocument26 pagesBiology Investigatory ProjectShruti LaskarNo ratings yet
- Corneoscleral T&S - PrinciplesDocument10 pagesCorneoscleral T&S - PrinciplesMuhammad SyamilNo ratings yet
- Clarastill™ Can-C (CE Approved As Medical Device) .Document1 pageClarastill™ Can-C (CE Approved As Medical Device) .dokter Hewan AdhonaNo ratings yet
- Current ConceptsDocument300 pagesCurrent ConceptsGuilherme Bender LimaNo ratings yet
- Lentile ScleraleDocument40 pagesLentile ScleraleLauraNo ratings yet
- Hifema: Classification and CharacteristicsDocument17 pagesHifema: Classification and CharacteristicsMarisa SukoNo ratings yet
- SOLIX Essential BrochureDocument12 pagesSOLIX Essential BrochureHaag-Streit UK (HS-UK)No ratings yet
- Asvs 04 0267Document7 pagesAsvs 04 0267T KNo ratings yet
- QP CODE: 2101: Section - A, AnatomyDocument122 pagesQP CODE: 2101: Section - A, AnatomyMeghanaNo ratings yet
- Microbial Keratitis Royal College of OphthalmologistDocument2 pagesMicrobial Keratitis Royal College of OphthalmologistmahadianNo ratings yet
- Corneal Ulcers in General Practice: Clinical IntelligenceDocument2 pagesCorneal Ulcers in General Practice: Clinical IntelligenceBenitaNo ratings yet
- Applanation TonometerDocument15 pagesApplanation TonometerMuhammed AbdulmajeedNo ratings yet