You might also like
- Refractive Management v1m1Document30 pagesRefractive Management v1m1Faisal AwaluddinNo ratings yet
- Max Eye Care Offers Precise LASIK Surgery With Fast RecoveryDocument2 pagesMax Eye Care Offers Precise LASIK Surgery With Fast RecoveryAstha JalanNo ratings yet
- Mertens - The Staar Toric ICLDocument4 pagesMertens - The Staar Toric ICLAndreea L. MihalceaNo ratings yet
- Cataract Surgery: Past-Present-FutureDocument44 pagesCataract Surgery: Past-Present-FutureNica Lopez FernandezNo ratings yet
- Referat SMILEDocument10 pagesReferat SMILEarumNo ratings yet
- Retinal Detachment ManagementDocument67 pagesRetinal Detachment ManagementHirendra VaishnavNo ratings yet
- Pre and Post Op Cataract EvaluaDocument56 pagesPre and Post Op Cataract Evaluahenok birukNo ratings yet
- Refractive SurgeryDocument56 pagesRefractive SurgeryMohiuddin AhmedNo ratings yet
- Are Intrastromal Treatments The Future of Refractive Surgery?Document11 pagesAre Intrastromal Treatments The Future of Refractive Surgery?lacisag100% (1)
- Surgeries for Refractory Errors of EyeDocument24 pagesSurgeries for Refractory Errors of EyeDestiny AttainNo ratings yet
- Enchancment After Cataract SurgeryDocument18 pagesEnchancment After Cataract SurgeryBrilliantineNo ratings yet
- Limbal Relaxing Incisions FixedDocument18 pagesLimbal Relaxing Incisions Fixedaswan bagasNo ratings yet
- Preparing For Cataract Surgery in Special Situations (Corneal Conditions and Compromised Visualization of The Lens)Document31 pagesPreparing For Cataract Surgery in Special Situations (Corneal Conditions and Compromised Visualization of The Lens)Hikban FiqhiNo ratings yet
- Visumax: Defining The Pulse Rate in Refractive SurgeryDocument16 pagesVisumax: Defining The Pulse Rate in Refractive Surgerykhairul ihsanNo ratings yet
- Principles of Vitreoretinal Surgery: Scleral Buckle TechniquesDocument49 pagesPrinciples of Vitreoretinal Surgery: Scleral Buckle TechniquesSriniwasNo ratings yet
- Update On Refractive SurgeryDocument15 pagesUpdate On Refractive SurgeryStefanieNo ratings yet
- Tugas Baca RS IndraDocument28 pagesTugas Baca RS IndraMade Surya DinajayaNo ratings yet
- 0210 f8 DanasouryDocument4 pages0210 f8 DanasouryLJANo ratings yet
- AOA Lasik Co-Management GuideDocument22 pagesAOA Lasik Co-Management GuideJitander DudeeNo ratings yet
- Lasik Technology Review in MalaysiaDocument20 pagesLasik Technology Review in Malaysiakey3hseNo ratings yet
- Jurnal Referat MataDocument8 pagesJurnal Referat MataWinda KristantiNo ratings yet
- Biometry..Iol CalculationDocument86 pagesBiometry..Iol CalculationSristi Thakur0% (1)
- Keratoplasty XDocument41 pagesKeratoplasty XArunimaNo ratings yet
- Photorefractive Keratectomy (PRK) Retreatment of Residual Refractive Errors After Laser in Situ Keratomileusis (LASIK)Document8 pagesPhotorefractive Keratectomy (PRK) Retreatment of Residual Refractive Errors After Laser in Situ Keratomileusis (LASIK)ayurNo ratings yet
- Keratoplasty: By: Esmaeil Hashemi MC: 410a Dept. of OphthalmologyDocument43 pagesKeratoplasty: By: Esmaeil Hashemi MC: 410a Dept. of OphthalmologyEsmaeil HashemiNo ratings yet
- Cryo, PDT & Wide Angle Fundus Camera: Presentor-Dr. Jay Singh Moderator - DR. Devashish SIRDocument46 pagesCryo, PDT & Wide Angle Fundus Camera: Presentor-Dr. Jay Singh Moderator - DR. Devashish SIRShahid ManzoorNo ratings yet
- Surgical Management of Senile CataractDocument39 pagesSurgical Management of Senile CataractKarthik ChellaNo ratings yet
- Comparision of Surgical Induced Astigmatism BetweeDocument5 pagesComparision of Surgical Induced Astigmatism BetweeHoly DishNo ratings yet
- Retinal Physician - Visualization in Vitrectomy - An UpdateDocument12 pagesRetinal Physician - Visualization in Vitrectomy - An UpdateDr. M. Hannan JamilNo ratings yet
- Retinal Detachment Surgery OutcomesDocument51 pagesRetinal Detachment Surgery OutcomesMuthulakshmiNo ratings yet
- Ocular Laser Therapy 12-5-14Document31 pagesOcular Laser Therapy 12-5-14Prasetiyo WilliamNo ratings yet
- Vitreous Prolapse ManagementDocument31 pagesVitreous Prolapse ManagementR.m. AndriyanNo ratings yet
- AAO Reading VitrectomyDocument65 pagesAAO Reading VitrectomydestiNo ratings yet
- The Benefits of Standardization in Laser Refractive SurgeryDocument4 pagesThe Benefits of Standardization in Laser Refractive SurgeryNabita AuliaNo ratings yet
- Sutureless single-port vitrectomy aids cataract surgeryDocument4 pagesSutureless single-port vitrectomy aids cataract surgeryasfwegereNo ratings yet
- Refractive Errors 3 2023Document32 pagesRefractive Errors 3 2023Vishwajeet RaneNo ratings yet
- Post-Keratoplasty Astigmatism Management by RelaxiDocument7 pagesPost-Keratoplasty Astigmatism Management by Relaximedamif3No ratings yet
- Safety and Efficacy of Low Energy Small Incision.33Document5 pagesSafety and Efficacy of Low Energy Small Incision.33dinimaslomanNo ratings yet
- Understanding LASIK Surgery a Comprehensive Guide to Laser Vision Correction.Document4 pagesUnderstanding LASIK Surgery a Comprehensive Guide to Laser Vision Correction.anileyehospitalNo ratings yet
- 21BOP012Document22 pages21BOP012avani vankarNo ratings yet
- USHM"REZONANCA"FAKULTETI I MJEKËSISË PRISHTINË/Halil AJVAZI/ReSTOR Patient Power Point/Ushtrimet..Document23 pagesUSHM"REZONANCA"FAKULTETI I MJEKËSISË PRISHTINË/Halil AJVAZI/ReSTOR Patient Power Point/Ushtrimet..HALIL Z.AJVAZI100% (1)
- 03 Refractive SurgeryDocument99 pages03 Refractive SurgeryWaqar Ahmad Khan100% (3)
- Femtosecond Laser Cataract Surgery - Magic or Myth? A Balanced View!Document31 pagesFemtosecond Laser Cataract Surgery - Magic or Myth? A Balanced View!RizkyAgustriaNo ratings yet
- Biometry: Dr. Sanjay Kumar SarkerDocument67 pagesBiometry: Dr. Sanjay Kumar SarkerNiloy Basak100% (3)
- Original Article Laser In-Situ Keratomileusis For Refractive Error Following Radial KeratotomyDocument4 pagesOriginal Article Laser In-Situ Keratomileusis For Refractive Error Following Radial KeratotomyngunhatNo ratings yet
- Astigmatic Change in Manual Small Incision Cataract Surgery (MSICS) With Chevron Type of IncisionDocument6 pagesAstigmatic Change in Manual Small Incision Cataract Surgery (MSICS) With Chevron Type of IncisionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ENT LESSON 8 (1)Document45 pagesENT LESSON 8 (1)favourednancie9No ratings yet
- SMILE Procedure GuideDocument8 pagesSMILE Procedure GuidearumNo ratings yet
- Management of Pediatric Cataract: (Preoperative, Intra and Postoperative)Document22 pagesManagement of Pediatric Cataract: (Preoperative, Intra and Postoperative)SIMRS RSUD KARAWANGNo ratings yet
- Keratoconus BCSCDocument27 pagesKeratoconus BCSCmedhanit anjuloNo ratings yet
- JurnalDocument21 pagesJurnalwidyastutiNo ratings yet
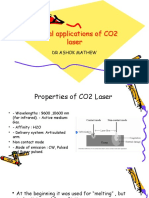
- CO2 Lasers NewDocument55 pagesCO2 Lasers NewlamaNo ratings yet
- Ijsrmjournal, Journal Manager, 17 IjsrmDocument9 pagesIjsrmjournal, Journal Manager, 17 IjsrmashishNo ratings yet
- COMPLICATIONS of CATARACT SURGERY (Capsular Opacification and Contraction and Hemorrhage)Document30 pagesCOMPLICATIONS of CATARACT SURGERY (Capsular Opacification and Contraction and Hemorrhage)Hikban Fiqhi100% (1)
- Small Incision Lenticule Extraction (SMILEDocument24 pagesSmall Incision Lenticule Extraction (SMILEarumNo ratings yet
- Lasik Center Report For IsoBeam D200Document9 pagesLasik Center Report For IsoBeam D200郭奕谷/Joey KuoNo ratings yet
- Types of Eye Surgery ProceduresDocument4 pagesTypes of Eye Surgery ProceduresJihad Elias ChahlaNo ratings yet
- Newer Trends in Lamellar Keratoplasty: Dr. Hijab MehtaDocument6 pagesNewer Trends in Lamellar Keratoplasty: Dr. Hijab MehtaNur Zulaekha Soraya YayaNo ratings yet
- Complications of MsicsDocument40 pagesComplications of MsicsSukhman kaur ButtarNo ratings yet
- Project ManagementDocument64 pagesProject Managementhenok birukNo ratings yet
- Pre and Post Op Cataract EvaluaDocument56 pagesPre and Post Op Cataract Evaluahenok birukNo ratings yet
- Advanced Glauc ManagmentDocument49 pagesAdvanced Glauc Managmenthenok birukNo ratings yet
- Retinopati Diabetik PDFDocument4 pagesRetinopati Diabetik PDFaulNo ratings yet
- Research Article: Diabetic Retinopathy in Native and Nonnative CanadiansDocument6 pagesResearch Article: Diabetic Retinopathy in Native and Nonnative Canadianshenok birukNo ratings yet
- CLV, VF Assessment 2021Document133 pagesCLV, VF Assessment 2021henok birukNo ratings yet
- L3 TelescopeDocument51 pagesL3 Telescopehenok birukNo ratings yet
- Clinical LV-Visual Impairment 2021Document60 pagesClinical LV-Visual Impairment 2021henok birukNo ratings yet
- Proposal Defence Presentation Template: Iph, UogDocument16 pagesProposal Defence Presentation Template: Iph, Uoghenok birukNo ratings yet
- Over View of Management For Optometry by ChalieDocument53 pagesOver View of Management For Optometry by Chaliehenok birukNo ratings yet
- CLV, VF Assessment 2021Document133 pagesCLV, VF Assessment 2021henok birukNo ratings yet
- Resource ManagementDocument90 pagesResource Managementhenok birukNo ratings yet
- Chapter 4 Introduction To ProbabilityDocument68 pagesChapter 4 Introduction To ProbabilityG Gጂጂ TubeNo ratings yet
- L2 Optical LV AidsDocument34 pagesL2 Optical LV Aidshenok birukNo ratings yet
- University of Gondar College of Medicine and Health Science Department of Epidemiology and BiostatisticsDocument34 pagesUniversity of Gondar College of Medicine and Health Science Department of Epidemiology and Biostatisticshenok birukNo ratings yet
- Chapter 1 IntroductionDocument30 pagesChapter 1 Introductionhenok birukNo ratings yet
- AR Sort Term Corneal Change-ZufanDocument31 pagesAR Sort Term Corneal Change-Zufanhenok birukNo ratings yet
- University of Gondar Estimation and Hypothesis TestingDocument119 pagesUniversity of Gondar Estimation and Hypothesis Testinghenok birukNo ratings yet
- Childhood Glaucoma NewDocument30 pagesChildhood Glaucoma Newhenok birukNo ratings yet
- ICRS Implantation Effectiveness for Keratoconus TreatmentDocument25 pagesICRS Implantation Effectiveness for Keratoconus Treatmenthenok birukNo ratings yet
- Chapter 2 Method of Data Collection andDocument59 pagesChapter 2 Method of Data Collection andG Gጂጂ TubeNo ratings yet
- AR Multifocal Orthok Vs Conventional in Mypoia Control-DessieDocument37 pagesAR Multifocal Orthok Vs Conventional in Mypoia Control-Dessiehenok birukNo ratings yet
- AR On SCCL For Adv. KCs-MeketeDocument24 pagesAR On SCCL For Adv. KCs-Meketehenok birukNo ratings yet
- AR Therapeutic CL - YohanisDocument35 pagesAR Therapeutic CL - Yohanishenok birukNo ratings yet
- A) Definition of Fusional ReservesDocument26 pagesA) Definition of Fusional Reserveshenok birukNo ratings yet
- AR Visual Performance BN DT CLs in KCs-BesufekadDocument19 pagesAR Visual Performance BN DT CLs in KCs-Besufekadhenok birukNo ratings yet
- AR Implantable Collamer Lens - HundumaDocument22 pagesAR Implantable Collamer Lens - Hundumahenok birukNo ratings yet
- ARContact Lens For Keratoconus - AmsaluDocument44 pagesARContact Lens For Keratoconus - Amsaluhenok birukNo ratings yet
- Heterophoria: University of Gondar Department of Optometry by Nebiyat FelekeDocument27 pagesHeterophoria: University of Gondar Department of Optometry by Nebiyat Felekehenok biruk100% (1)
- The Host Is Getting Beautiful Every Day 251-300Document194 pagesThe Host Is Getting Beautiful Every Day 251-300HET SHETHNo ratings yet
- Behavioral optometryDocument316 pagesBehavioral optometryCHIMA ONWUKA MONGNo ratings yet
- OSCE - Cranial Nerve ExaminationDocument2 pagesOSCE - Cranial Nerve ExaminationA.C.No ratings yet
- Scleral Lenses: Presented By: Umair WakeelDocument39 pagesScleral Lenses: Presented By: Umair WakeelXid KhanNo ratings yet
- Makeup Consultation FormDocument2 pagesMakeup Consultation Formapi-339347949100% (1)
- Contingency ProcedureDocument27 pagesContingency ProcedureRoldan Dela CruzNo ratings yet
- Strabismus For Med VDocument102 pagesStrabismus For Med Vhenok birukNo ratings yet
- Safety Data Sheet Servisol Silicone Sealant: 1. Identification of The Substance/Preparation and The CompanyDocument4 pagesSafety Data Sheet Servisol Silicone Sealant: 1. Identification of The Substance/Preparation and The CompanyFseha GetahunNo ratings yet
- Tgas Bahasa InggrisDocument2 pagesTgas Bahasa Inggrisbilly jordiNo ratings yet
- Dr Jusuf Wijaya , SpM FK - UKI Cawang Curriculum Vitae and Specialization in StrabismusDocument32 pagesDr Jusuf Wijaya , SpM FK - UKI Cawang Curriculum Vitae and Specialization in StrabismusGerry SanjayaNo ratings yet
- Research & Evidence For Sports Vision: by Steve Leslie Boptom, Leonard Press Od & Mark Overton December 2016Document4 pagesResearch & Evidence For Sports Vision: by Steve Leslie Boptom, Leonard Press Od & Mark Overton December 2016Evelyn SepulvedaNo ratings yet
- Symptoms & Remedies For Dry EyesDocument6 pagesSymptoms & Remedies For Dry Eyeshatime alouiNo ratings yet
- HSB Endocrine System and EyeDocument15 pagesHSB Endocrine System and EyeNisha JodhanNo ratings yet
- Times Leader 01-17-2012Document32 pagesTimes Leader 01-17-2012The Times LeaderNo ratings yet
- Research Article: (Occlu-Pad) DeviceDocument5 pagesResearch Article: (Occlu-Pad) Devicearyo aryoNo ratings yet
- Modern Marvels or New Nasties?Document4 pagesModern Marvels or New Nasties?Emilija KrivegaiteNo ratings yet
- Dormex MSDSDocument10 pagesDormex MSDSAghilesNo ratings yet
- Manual - DeWalt 7485 Table SawDocument44 pagesManual - DeWalt 7485 Table SawJ PNo ratings yet
- WB 2 Body Face Routines Wellbox Men enDocument11 pagesWB 2 Body Face Routines Wellbox Men enAlan BishopNo ratings yet
- Comparative Advantage Interview Questions FinalDocument6 pagesComparative Advantage Interview Questions Finalapi-503034798No ratings yet
- Safe installation of PV systems according to OSHA regulationsDocument7 pagesSafe installation of PV systems according to OSHA regulationsSolar - Marketing/CELNo ratings yet
- Ocular Trauma Lecture MBBS by Prof Munim SuriDocument60 pagesOcular Trauma Lecture MBBS by Prof Munim SuriMunim SuriNo ratings yet
- Evaluation of Total Corneal Power MeasurementsDocument7 pagesEvaluation of Total Corneal Power MeasurementsMariana Luzardo bravoNo ratings yet
- Resume Nasogastric Tube InstallationDocument17 pagesResume Nasogastric Tube InstallationRedmy LasmanaNo ratings yet
- MEHT130423 - Information For Screening For Retinopathy of Prematurity 1.0Document4 pagesMEHT130423 - Information For Screening For Retinopathy of Prematurity 1.0Rohit BharadwajNo ratings yet
- Do's and Don'ts For Wearing Contact LensDocument1 pageDo's and Don'ts For Wearing Contact LensMrkikuNo ratings yet
- LNGI-RA-HEC-398-Fabrication Works (Welding, Cutting, Grinding, Drilling, Threading, Support, and Power Tools Operations) Rev.3Document2 pagesLNGI-RA-HEC-398-Fabrication Works (Welding, Cutting, Grinding, Drilling, Threading, Support, and Power Tools Operations) Rev.3Ramesh arumugam0% (1)
- Clinical Management of Binocular Vision .24Document1 pageClinical Management of Binocular Vision .24Ikmal ShahromNo ratings yet
- ConjunctivitisDocument9 pagesConjunctivitisSaranya DeviNo ratings yet
- Aero-Technology - Dgca & Easa Module 9 - Human Factors Questions - Part-1Document20 pagesAero-Technology - Dgca & Easa Module 9 - Human Factors Questions - Part-1renjithaeroNo ratings yet