You might also like
- Comprehensive Geriatric AssessmentDocument87 pagesComprehensive Geriatric AssessmentNurrahmanita AzizaNo ratings yet
- Modelo Baja VisionDocument24 pagesModelo Baja VisioneveNo ratings yet
- How To Evaluate An ArticleDocument38 pagesHow To Evaluate An ArticleSenaa DaughterNo ratings yet
- Clinical LV-Visual Impairment 2021Document60 pagesClinical LV-Visual Impairment 2021henok birukNo ratings yet
- Remediating The Struggling ResidentDocument52 pagesRemediating The Struggling Residentomegasauron0gmailcomNo ratings yet
- CLT 23-24 - Dr. Helmia Hasan - Eval - Feedback 14 Nov 2022Document52 pagesCLT 23-24 - Dr. Helmia Hasan - Eval - Feedback 14 Nov 2022bbj4bqpwf5No ratings yet
- Better Handoffs. Safer CareDocument49 pagesBetter Handoffs. Safer CareSatanan DamrisuNo ratings yet
- Clinical Management of Cognitive Impairment After COVIDDocument200 pagesClinical Management of Cognitive Impairment After COVIDJeanine Angela CuliliNo ratings yet
- NUR 326 Gerontological Nursing-StudyGuideExam1-Spring2023Document3 pagesNUR 326 Gerontological Nursing-StudyGuideExam1-Spring2023Cristina CebanuNo ratings yet
- UNIT - 1 - Prognosis Research - IntroductionDocument80 pagesUNIT - 1 - Prognosis Research - Introductiontila12negaNo ratings yet
- Children With Visual ImpairmentDocument35 pagesChildren With Visual Impairmentkobby klausNo ratings yet
- FU-M1-CU5 LEC Nursing Diagnosis - Utilizing Nurse's Reasoning ProcessDocument9 pagesFU-M1-CU5 LEC Nursing Diagnosis - Utilizing Nurse's Reasoning ProcessBig DaddyNo ratings yet
- Ophthalmic Evaluation & Approaches To The PatientDocument11 pagesOphthalmic Evaluation & Approaches To The PatientDesra AufarNo ratings yet
- Understanding Low Vision Terms for Optometric PracticeDocument27 pagesUnderstanding Low Vision Terms for Optometric PracticeJohn DeanNo ratings yet
- SBARQ FormDocument1 pageSBARQ FormTracy100% (5)
- Cognitive and Perceputal ImpairmentsDocument88 pagesCognitive and Perceputal ImpairmentsMangala Prema MohanarangamNo ratings yet
- VI pptDocument55 pagesVI pptTadesse TedlaNo ratings yet
- Ophthalmic Evaluation & Approaches To The PatientDocument11 pagesOphthalmic Evaluation & Approaches To The PatientChandraNo ratings yet
- Red Eye Diagnosis & Treatment GuideDocument10 pagesRed Eye Diagnosis & Treatment GuideFaith LoveNo ratings yet
- Modules 9 10Document12 pagesModules 9 10Callie ParkNo ratings yet
- University of Gondar Cmhs Department of Optometry: BV and Clinical NeurologyDocument36 pagesUniversity of Gondar Cmhs Department of Optometry: BV and Clinical NeurologyGetenet shumetNo ratings yet
- Annex A: Year 5 Learning OutcomesDocument9 pagesAnnex A: Year 5 Learning OutcomeslukesqueNo ratings yet
- Functional Vision AssessmentDocument17 pagesFunctional Vision AssessmentKavi RehabianNo ratings yet
- Formulation of Study Variables & Research ObjectivesDocument21 pagesFormulation of Study Variables & Research Objectivescy lifeNo ratings yet
- Melville-Nelson Self-Care Assessment-2Document26 pagesMelville-Nelson Self-Care Assessment-2api-239817112No ratings yet
- 1-Introduction To Pediatric OptometryDocument14 pages1-Introduction To Pediatric OptometryAmrNo ratings yet
- SS 2Document29 pagesSS 2JamNo ratings yet
- Examination & Diagnosis of Edentulous Patients: Presented By: Dr. Jehan Dordi 1 Yr. MdsDocument159 pagesExamination & Diagnosis of Edentulous Patients: Presented By: Dr. Jehan Dordi 1 Yr. MdsAkanksha MahajanNo ratings yet
- Orientation, History Taking and ExaminationDocument77 pagesOrientation, History Taking and ExaminationMuhammad AwaisNo ratings yet
- Postconcussive Syndrome (PCS) Clinical Practice Guideline: Occupational TherapyDocument7 pagesPostconcussive Syndrome (PCS) Clinical Practice Guideline: Occupational TherapyNicoleta Stoica100% (1)
- Cortical Visual Impairment Rehabilitation StrategiesDocument55 pagesCortical Visual Impairment Rehabilitation StrategiesIntanOktavianaAdiyanto100% (1)
- 1 骨科 Fundamentals of Musculoskeletal Physical Therapy 講義Document33 pages1 骨科 Fundamentals of Musculoskeletal Physical Therapy 講義林芝生No ratings yet
- Visual StanderdsDocument31 pagesVisual StanderdsEmaan NoorNo ratings yet
- Sample Competency Assessment ToolDocument10 pagesSample Competency Assessment ToolHengkyNo ratings yet
- Retraso Del DesarrolloDocument47 pagesRetraso Del DesarrolloPaola BGNo ratings yet
- Care of Clients With Alterations in Cognitive-Perceptual PatternsDocument98 pagesCare of Clients With Alterations in Cognitive-Perceptual PatternsRose Anne Riotoc BarrientosNo ratings yet
- Low Vision in ChildrenDocument22 pagesLow Vision in Childrenfari_rose42807No ratings yet
- Book 4Document3 pagesBook 4Vikram Raj SinghNo ratings yet
- Low Vision PrinciplesDocument272 pagesLow Vision Principlesmariam mhNo ratings yet
- Geriatric Scales SPIDocument20 pagesGeriatric Scales SPIsanavoraNo ratings yet
- 07 - Visual Rehabilitation For Diabetic RetinopathyDocument16 pages07 - Visual Rehabilitation For Diabetic Retinopathyssha_szaimiNo ratings yet
- The Vineland Adaptive Behavior ScalesDocument2 pagesThe Vineland Adaptive Behavior ScalesBuro GroupNo ratings yet
- LOW VISION EXAMINAION EditedDocument16 pagesLOW VISION EXAMINAION EditedANN ANABANo ratings yet
- SKI MKT. 470 Ch. 5Document19 pagesSKI MKT. 470 Ch. 5MST. Sabina Parvin 1330122030No ratings yet
- Clinical Decision Making Process in PTDocument50 pagesClinical Decision Making Process in PTNoor Ul-ainNo ratings yet
- Cognitive Symptoms Guidance Tables 030222Document10 pagesCognitive Symptoms Guidance Tables 030222Sudarshana DasguptaNo ratings yet
- Advanced Glauc ManagmentDocument49 pagesAdvanced Glauc Managmenthenok birukNo ratings yet
- 1.CATARACTDocument31 pages1.CATARACTsnehalNo ratings yet
- Student__PPN 102 W24 Week 4 Nursing Process P1Document44 pagesStudent__PPN 102 W24 Week 4 Nursing Process P1phuongphuonganhanh171203No ratings yet
- 13.4. Diagnosis Tumbuh KembangDocument33 pages13.4. Diagnosis Tumbuh KembangMuhammad Ilham KhatamiNo ratings yet
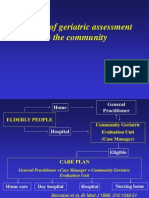
- The Use of Geriatric Assessment in The CommunityDocument16 pagesThe Use of Geriatric Assessment in The Communityhendra2darmawanNo ratings yet
- Rehabilitation in Visual and Hearing Disability: Prof. Dr. Dr. Widjajalaksmi K., SPKFR (K), MSCDocument44 pagesRehabilitation in Visual and Hearing Disability: Prof. Dr. Dr. Widjajalaksmi K., SPKFR (K), MSCHeQta SSNo ratings yet
- DIARY ncm114 NamoroGr2Document2 pagesDIARY ncm114 NamoroGr2John Lloyd NamoroNo ratings yet
- Aniketh CV1Document2 pagesAniketh CV1Jean HarveyNo ratings yet
- Assessing Low Vision FunctionDocument65 pagesAssessing Low Vision FunctionNikola MarsenicNo ratings yet
- Career Counseling For People With Vision LossDocument48 pagesCareer Counseling For People With Vision LossArash HalimNo ratings yet
- Head to toe assessmentDocument34 pagesHead to toe assessmentsofiamansoorNo ratings yet
- Nursing Process 2020 - 20-1-20Document25 pagesNursing Process 2020 - 20-1-20Zubda ButtNo ratings yet
- A D.O. Student's Guide To Residency: Where Does It End?Document155 pagesA D.O. Student's Guide To Residency: Where Does It End?Blessing KelechiNo ratings yet
- Advanced Glauc ManagmentDocument49 pagesAdvanced Glauc Managmenthenok birukNo ratings yet
- Pre and Post Op Cataract EvaluaDocument56 pagesPre and Post Op Cataract Evaluahenok birukNo ratings yet
- Research Article: Diabetic Retinopathy in Native and Nonnative CanadiansDocument6 pagesResearch Article: Diabetic Retinopathy in Native and Nonnative Canadianshenok birukNo ratings yet
- Retinopati Diabetik PDFDocument4 pagesRetinopati Diabetik PDFaulNo ratings yet
- Proposal Defence Presentation Template: Iph, UogDocument16 pagesProposal Defence Presentation Template: Iph, Uoghenok birukNo ratings yet
- CLV, VF Assessment 2021Document133 pagesCLV, VF Assessment 2021henok birukNo ratings yet
- L2 Optical LV AidsDocument34 pagesL2 Optical LV Aidshenok birukNo ratings yet
- Project ManagementDocument64 pagesProject Managementhenok birukNo ratings yet
- Chapter 2 Method of Data Collection andDocument59 pagesChapter 2 Method of Data Collection andG Gጂጂ TubeNo ratings yet
- Over View of Management For Optometry by ChalieDocument53 pagesOver View of Management For Optometry by Chaliehenok birukNo ratings yet
- Resource ManagementDocument90 pagesResource Managementhenok birukNo ratings yet
- AR Refractive Surgery-KalkidanDocument47 pagesAR Refractive Surgery-Kalkidanhenok birukNo ratings yet
- L3 TelescopeDocument51 pagesL3 Telescopehenok birukNo ratings yet
- University of Gondar College of Medicine and Health Science Department of Epidemiology and BiostatisticsDocument34 pagesUniversity of Gondar College of Medicine and Health Science Department of Epidemiology and Biostatisticshenok birukNo ratings yet
- Chapter 4 Introduction To ProbabilityDocument68 pagesChapter 4 Introduction To ProbabilityG Gጂጂ TubeNo ratings yet
- University of Gondar Estimation and Hypothesis TestingDocument119 pagesUniversity of Gondar Estimation and Hypothesis Testinghenok birukNo ratings yet
- AR On SCCL For Adv. KCs-MeketeDocument24 pagesAR On SCCL For Adv. KCs-Meketehenok birukNo ratings yet
- ICRS Implantation Effectiveness for Keratoconus TreatmentDocument25 pagesICRS Implantation Effectiveness for Keratoconus Treatmenthenok birukNo ratings yet
- AR Implantable Collamer Lens - HundumaDocument22 pagesAR Implantable Collamer Lens - Hundumahenok birukNo ratings yet
- Chapter 1 IntroductionDocument30 pagesChapter 1 Introductionhenok birukNo ratings yet
- AR Multifocal Orthok Vs Conventional in Mypoia Control-DessieDocument37 pagesAR Multifocal Orthok Vs Conventional in Mypoia Control-Dessiehenok birukNo ratings yet
- Childhood Glaucoma NewDocument30 pagesChildhood Glaucoma Newhenok birukNo ratings yet
- A) Definition of Fusional ReservesDocument26 pagesA) Definition of Fusional Reserveshenok birukNo ratings yet
- AR Sort Term Corneal Change-ZufanDocument31 pagesAR Sort Term Corneal Change-Zufanhenok birukNo ratings yet
- AR Therapeutic CL - YohanisDocument35 pagesAR Therapeutic CL - Yohanishenok birukNo ratings yet
- Heterophoria: University of Gondar Department of Optometry by Nebiyat FelekeDocument27 pagesHeterophoria: University of Gondar Department of Optometry by Nebiyat Felekehenok biruk100% (1)
- AR Visual Performance BN DT CLs in KCs-BesufekadDocument19 pagesAR Visual Performance BN DT CLs in KCs-Besufekadhenok birukNo ratings yet
- ARContact Lens For Keratoconus - AmsaluDocument44 pagesARContact Lens For Keratoconus - Amsaluhenok birukNo ratings yet
- Coaching, Mentoring & OnboardingDocument43 pagesCoaching, Mentoring & OnboardingosvehNo ratings yet
- Strawberry GenerationDocument2 pagesStrawberry GenerationImat12No ratings yet
- The Greatest Showman PDFDocument22 pagesThe Greatest Showman PDFMJ RecordNo ratings yet
- The Dogon Tribe of The Sirius MysteryDocument5 pagesThe Dogon Tribe of The Sirius MysteryLaron Clark100% (1)
- Compiler Design and Linux System AdministrationDocument47 pagesCompiler Design and Linux System AdministrationGouri ShankerNo ratings yet
- Direct Marketing: Mcgraw-Hill/IrwinDocument30 pagesDirect Marketing: Mcgraw-Hill/IrwinJunaid KhalidNo ratings yet
- MKTM028 FathimathDocument23 pagesMKTM028 FathimathShyamly DeepuNo ratings yet
- Master in Public Management: Application PacketDocument6 pagesMaster in Public Management: Application PacketMark GironNo ratings yet
- Sharp Sharp Cash Register Xe A207 Users Manual 284068Document1 pageSharp Sharp Cash Register Xe A207 Users Manual 284068Zeila CordeiroNo ratings yet
- Ffective Riting Kills: Training & Discussion OnDocument37 pagesFfective Riting Kills: Training & Discussion OnKasi ReddyNo ratings yet
- Knowledge Paper XDocument28 pagesKnowledge Paper XLaurențiu Cătălin NeagoeNo ratings yet
- Ruach Ha Kodesh or Holy Religious SpiritDocument10 pagesRuach Ha Kodesh or Holy Religious Spiritharsan100% (1)
- Pag-IBIG Employer Enrollment FormDocument1 pagePag-IBIG Employer Enrollment FormDarlyn Etang100% (1)
- The Historical Foundations of Law. Harold BermanDocument13 pagesThe Historical Foundations of Law. Harold BermanespinasdorsalesNo ratings yet
- Role of Therapeutic Gardens in Healthy Cities: Design StandardsDocument3 pagesRole of Therapeutic Gardens in Healthy Cities: Design Standardsaarthi SureshNo ratings yet
- How To VOR WorksDocument23 pagesHow To VOR WorksHai AuNo ratings yet
- Pediatrics Study ScheduleDocument2 pagesPediatrics Study ScheduleNatnaelNo ratings yet
- MPMC All Questions and AnswerDocument6 pagesMPMC All Questions and AnswerMODERN TELUGAMMAYINo ratings yet
- The Korean MiracleDocument20 pagesThe Korean MiracleDivya GirishNo ratings yet
- Foundations On Expansive Soils: 3.1. BackgroundDocument31 pagesFoundations On Expansive Soils: 3.1. BackgroundbiniNo ratings yet
- Self-Sustainable Village: Dharm Raj Jangid 16031AA015Document2 pagesSelf-Sustainable Village: Dharm Raj Jangid 16031AA015Dharm JangidNo ratings yet
- PDA Technical Documents on Sterilization ProcessesDocument3 pagesPDA Technical Documents on Sterilization ProcessesManas MishraNo ratings yet
- PDI 14 Asthma Admission RateDocument2 pagesPDI 14 Asthma Admission RatejrmyfngNo ratings yet
- Segmentation: NIVEA Sun Case Study Summary Downloaded From The Times 100 Edition 11Document2 pagesSegmentation: NIVEA Sun Case Study Summary Downloaded From The Times 100 Edition 11Boon-Pin NgNo ratings yet
- Albert Einstein - Wikipedia, The Free EncyclopediaDocument34 pagesAlbert Einstein - Wikipedia, The Free EncyclopediaalhanunNo ratings yet
- Actor analysis explores decision-making in environmental governanceDocument48 pagesActor analysis explores decision-making in environmental governancerizkyNo ratings yet
- Presentation on Indentured LabourersDocument10 pagesPresentation on Indentured LabourersAshis karmakar100% (1)
- Training Programme EvaluationDocument14 pagesTraining Programme Evaluationthanhloan1902No ratings yet
- Using Previous Years AlmanacDocument1 pageUsing Previous Years AlmanacbhabhasunilNo ratings yet