You might also like
- Surgical Management of Senile CataractDocument39 pagesSurgical Management of Senile CataractKarthik ChellaNo ratings yet
- Tugas Baca RS IndraDocument28 pagesTugas Baca RS IndraMade Surya DinajayaNo ratings yet
- AR Refractive Surgery-KalkidanDocument47 pagesAR Refractive Surgery-Kalkidanhenok birukNo ratings yet
- Small Incision Lenticule Extraction (SMILEDocument24 pagesSmall Incision Lenticule Extraction (SMILEarumNo ratings yet
- Senile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsDocument5 pagesSenile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsAhmad FahroziNo ratings yet
- PhacoemulsificationDocument54 pagesPhacoemulsificationIshita Kinra100% (1)
- Small Incision Cataract SurgeryDocument8 pagesSmall Incision Cataract Surgerykefi998100% (3)
- 0210 f8 DanasouryDocument4 pages0210 f8 DanasouryLJANo ratings yet
- Vitreous Prolapse ManagementDocument31 pagesVitreous Prolapse ManagementR.m. AndriyanNo ratings yet
- Correcting Astigmatism with Toric IOLsDocument28 pagesCorrecting Astigmatism with Toric IOLsArif MohammadNo ratings yet
- Cataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkDocument33 pagesCataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkvladimanpeNo ratings yet
- Baru Mata 2Document29 pagesBaru Mata 2Ichsan DiazNo ratings yet
- Oculofacial Plastic and Orbital SurgeryDocument14 pagesOculofacial Plastic and Orbital SurgeryTakwinNo ratings yet
- Referat SMILEDocument10 pagesReferat SMILEarumNo ratings yet
- Basic VitrectomyDocument24 pagesBasic Vitrectomykomitemedik.rsudsdaNo ratings yet
- Cataract 2 Lecture MBBS by Prof Munim SuriDocument37 pagesCataract 2 Lecture MBBS by Prof Munim SuriMunim SuriNo ratings yet
- Mertens - The Staar Toric ICLDocument4 pagesMertens - The Staar Toric ICLAndreea L. MihalceaNo ratings yet
- Newer Trends in Lamellar Keratoplasty: Dr. Hijab MehtaDocument6 pagesNewer Trends in Lamellar Keratoplasty: Dr. Hijab MehtaNur Zulaekha Soraya YayaNo ratings yet
- Intacs: By-Dr. Shirish Patel Moderator - Dr. Mukesh ParyaniDocument16 pagesIntacs: By-Dr. Shirish Patel Moderator - Dr. Mukesh ParyanineovisioncareNo ratings yet
- Keratoplasty: By: Esmaeil Hashemi MC: 410a Dept. of OphthalmologyDocument43 pagesKeratoplasty: By: Esmaeil Hashemi MC: 410a Dept. of OphthalmologyEsmaeil HashemiNo ratings yet
- Basic Manual Small Incision Cataract Surgery: Dr. Cok I Dewiyani, SP.MDocument65 pagesBasic Manual Small Incision Cataract Surgery: Dr. Cok I Dewiyani, SP.MCok Krishna D. PemayunNo ratings yet
- Modified Sewing Machine Technique For IridodialysiDocument8 pagesModified Sewing Machine Technique For IridodialysiRonal PerinoNo ratings yet
- SICS Cataract Surgery Complications PreventionDocument9 pagesSICS Cataract Surgery Complications Preventioninna_luv_u9006No ratings yet
- Keratoplasty XDocument41 pagesKeratoplasty XArunimaNo ratings yet
- Are Intrastromal Treatments The Future of Refractive Surgery?Document11 pagesAre Intrastromal Treatments The Future of Refractive Surgery?lacisag100% (1)
- Repair of Eyelid Laceration: Dr. Rashmi Joshi DNB Student BceircDocument49 pagesRepair of Eyelid Laceration: Dr. Rashmi Joshi DNB Student BceircPraful ChaudharyNo ratings yet
- Adenoidectomy and Tosillectomy MethodsDocument5 pagesAdenoidectomy and Tosillectomy MethodsBkas GrgNo ratings yet
- 05 EcceDocument9 pages05 EccebebibebihoNo ratings yet
- Cataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkDocument33 pagesCataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkVigneshNo ratings yet
- Comparision of Surgical Induced Astigmatism BetweeDocument5 pagesComparision of Surgical Induced Astigmatism BetweeHoly DishNo ratings yet
- Anterior VitrectomyDocument6 pagesAnterior VitrectomyEdward Alexander Lindo RojasNo ratings yet
- Guide to Intraocular Cataract Extraction Techniques (ICCE ECCEDocument61 pagesGuide to Intraocular Cataract Extraction Techniques (ICCE ECCEBboy ToonNo ratings yet
- Eye ProblemsDocument25 pagesEye ProblemsHikmat UllahNo ratings yet
- Nylon LoopDocument4 pagesNylon LooporlandgpicadoNo ratings yet
- Cataract 20surgery 2029 05 2008 131224024457 Phpapp01Document61 pagesCataract 20surgery 2029 05 2008 131224024457 Phpapp01sachin48No ratings yet
- (123doc) Opthalmic Microsurgical Suturing Techniques Part 7Document15 pages(123doc) Opthalmic Microsurgical Suturing Techniques Part 7TEODORA MIHAELA PELEASANo ratings yet
- Trabeculectomy Procedure for Lowering Eye PressureDocument42 pagesTrabeculectomy Procedure for Lowering Eye PressureAnita Zhang100% (1)
- Bab III Fako ReferatDocument2 pagesBab III Fako ReferatSartini Roma Dame NainggolanNo ratings yet
- Pershing 2011Document6 pagesPershing 2011asfwegereNo ratings yet
- Pi Is 1319453411000580Document5 pagesPi Is 1319453411000580Hario Tri HendrokoNo ratings yet
- Trocar Surgery for Cataract Surgeons: From Dislocated IOL to Dropped NucleusFrom EverandTrocar Surgery for Cataract Surgeons: From Dislocated IOL to Dropped NucleusNo ratings yet
- New Technique of Deep Anterior Lamellar KeratoplastyDocument5 pagesNew Technique of Deep Anterior Lamellar KeratoplastyLeonardo TorquettiNo ratings yet
- 06 Small Incision Cataract SurgeryDocument21 pages06 Small Incision Cataract SurgeryApriliani SanitiNo ratings yet
- Pars Plana Vitrectomy PDFDocument12 pagesPars Plana Vitrectomy PDFAvluz AdiansuhNo ratings yet
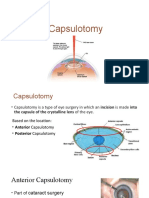
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlNo ratings yet
- Evisceration With Autogenous Scleral Graft and Bioceramic Implantation Within The Modified Scleral Shell 133 Cases Over 17 YearsDocument6 pagesEvisceration With Autogenous Scleral Graft and Bioceramic Implantation Within The Modified Scleral Shell 133 Cases Over 17 YearsSaraelsy MonterrosoNo ratings yet
- E-ISSN 0976-2892 Techniques Repair of Iris DefectsDocument2 pagesE-ISSN 0976-2892 Techniques Repair of Iris DefectsRajinder Kumar BassanNo ratings yet
- Flap Konjungtiva SusanDocument10 pagesFlap Konjungtiva SusanGlaucoma UnhasNo ratings yet
- GlaucomaDocument24 pagesGlaucomayousifNo ratings yet
- Scleral Fixated Intraocular Lens Implantation - A Comprehensive ReviewDocument25 pagesScleral Fixated Intraocular Lens Implantation - A Comprehensive ReviewBhumika RathNo ratings yet
- Devgan. Phaco Fundamentals. BookDocument29 pagesDevgan. Phaco Fundamentals. Bookjuanjorlopez100% (3)
- Exploring and Understanding The Benefits of Torsional PhacoemulsificationDocument13 pagesExploring and Understanding The Benefits of Torsional Phacoemulsificationthubui90No ratings yet
- Phakic Iol: Dr. Gauree GattaniDocument59 pagesPhakic Iol: Dr. Gauree GattaniArif MohammadNo ratings yet
- Cataract Coach BookDocument62 pagesCataract Coach Bookravian8bNo ratings yet
- Sutureless single-port vitrectomy aids cataract surgeryDocument4 pagesSutureless single-port vitrectomy aids cataract surgeryasfwegereNo ratings yet
- Zepto-Rhexis IndianJOphthalmol 2018Document4 pagesZepto-Rhexis IndianJOphthalmol 2018dwongNo ratings yet
- Dropped Nucleus ManagementDocument32 pagesDropped Nucleus ManagementNiloy Basak100% (2)
- Prosthesis, Appliances For Eye and Recent AdvancesDocument32 pagesProsthesis, Appliances For Eye and Recent AdvancesShivaramanRamachandranNo ratings yet
- The role of nurses in cataract diagnosis, surgery and aftercareDocument5 pagesThe role of nurses in cataract diagnosis, surgery and aftercareFara Sakina RahmaNo ratings yet
- SCAAREDAdultVersion 1.19.18-1Document3 pagesSCAAREDAdultVersion 1.19.18-1Nica Lopez FernandezNo ratings yet
- Biochem CBDocument114 pagesBiochem CBNica Lopez FernandezNo ratings yet
- 00009Document3 pages00009Nica Lopez FernandezNo ratings yet
- 00061Document3 pages00061Nica Lopez FernandezNo ratings yet
- Stesso - BotoxDocument5 pagesStesso - BotoxNica Lopez FernandezNo ratings yet
- Cellular Signal TransductionDocument10 pagesCellular Signal TransductionNica Lopez FernandezNo ratings yet
- RDO No. 39 - South Quezon CityDocument376 pagesRDO No. 39 - South Quezon CityNotario PrivadoNo ratings yet
- LIPOPROTEINS They Are The TransportersDocument25 pagesLIPOPROTEINS They Are The TransportersNica Lopez FernandezNo ratings yet
- CBBR ObDocument63 pagesCBBR ObNica Lopez FernandezNo ratings yet
- Glucose-6-Phosphate Is Also Known As A Central Metabolite Because It Can Enter A Lot of PathwaysDocument10 pagesGlucose-6-Phosphate Is Also Known As A Central Metabolite Because It Can Enter A Lot of PathwaysNica Lopez FernandezNo ratings yet
- Hernia Questions ExplainedDocument6 pagesHernia Questions ExplainedNica Lopez FernandezNo ratings yet
- Biochem A Porphyrin and Respiration - Dr. Bravo Hemoglobin CharacteristicsDocument9 pagesBiochem A Porphyrin and Respiration - Dr. Bravo Hemoglobin CharacteristicsNica Lopez FernandezNo ratings yet
- Hemothorax: PGI FACTORAN, Michelle Pgi Fernandez, JennicaDocument6 pagesHemothorax: PGI FACTORAN, Michelle Pgi Fernandez, JennicaNica Lopez FernandezNo ratings yet
- Stomach QuestionsDocument4 pagesStomach QuestionsNica Lopez FernandezNo ratings yet
- PNEUMONIA: Phases, Manifestations, and DiagnosisDocument47 pagesPNEUMONIA: Phases, Manifestations, and DiagnosisNica Lopez FernandezNo ratings yet
- Physician Licensure Exam Covers BiochemistryDocument178 pagesPhysician Licensure Exam Covers BiochemistryNica Lopez FernandezNo ratings yet
- Schizophrenia 2Document68 pagesSchizophrenia 2Nica Lopez FernandezNo ratings yet
- Urinary Tract Infection: PGI FRANCISCO, Maria Ellaine Pgi Galvez, AngeloDocument74 pagesUrinary Tract Infection: PGI FRANCISCO, Maria Ellaine Pgi Galvez, AngeloNica Lopez FernandezNo ratings yet
- PLE March 2019 RecallDocument10 pagesPLE March 2019 RecallNica Lopez FernandezNo ratings yet
- Physician Licensure Exam March 2019 Recall NotesDocument4 pagesPhysician Licensure Exam March 2019 Recall NotesNica Lopez FernandezNo ratings yet
- Physician Licensure Exam Covers BiochemistryDocument178 pagesPhysician Licensure Exam Covers BiochemistryNica Lopez FernandezNo ratings yet
- Reastaurant Near Moa - Google Search PDFDocument1 pageReastaurant Near Moa - Google Search PDFNica Lopez FernandezNo ratings yet
- PLE September 2016 RecallDocument7 pagesPLE September 2016 RecallNica Lopez FernandezNo ratings yet
- Board-Exam-Recall 2017Document109 pagesBoard-Exam-Recall 2017Nica Lopez FernandezNo ratings yet
- Extracapsular Cataract Extraction (Ecce)Document9 pagesExtracapsular Cataract Extraction (Ecce)Nica Lopez FernandezNo ratings yet
- Cataract Surgery and CodingDocument25 pagesCataract Surgery and CodingNica Lopez FernandezNo ratings yet
- Board Questions As RecalledDocument13 pagesBoard Questions As RecalledLian Baylosis100% (1)
- SCHIZOPHRENIA: A Clinical Syndrome of Variable PsychopathologyDocument7 pagesSCHIZOPHRENIA: A Clinical Syndrome of Variable PsychopathologyNica Lopez FernandezNo ratings yet
- Pre and Post Operative Management of Cataract Surgery: Pabita Dhungel B.OptometryDocument47 pagesPre and Post Operative Management of Cataract Surgery: Pabita Dhungel B.OptometryNica Lopez FernandezNo ratings yet
- The Eye Guide Matching 1Document75 pagesThe Eye Guide Matching 1trisna minNo ratings yet
- Leukocoria - StatPearls - Rak Buku NCBIDocument1 pageLeukocoria - StatPearls - Rak Buku NCBIbeby febyola siagianNo ratings yet
- Ophthalmic Disease Homoeopathic GuideDocument15 pagesOphthalmic Disease Homoeopathic GuideJhakhar WelfareSocietyNo ratings yet
- Diseases of The Uveal Tract 09Document24 pagesDiseases of The Uveal Tract 09somebody_ma100% (7)
- Your Health: The Annual Physician & Health Care DirectoryDocument49 pagesYour Health: The Annual Physician & Health Care DirectorykschofieldNo ratings yet
- Hesi Med Surg Study GuideDocument1 pageHesi Med Surg Study GuideGeorgeNo ratings yet
- DT LeukocoriaDocument44 pagesDT LeukocoriahamzahNo ratings yet
- Impact of The Possible Prognostic Factors For Visual OutcomesDocument11 pagesImpact of The Possible Prognostic Factors For Visual OutcomesBima RizkiNo ratings yet
- Cbleenpl 11Document12 pagesCbleenpl 11Jeeva JohnNo ratings yet
- Sudha N: Retina Wellness Report For Blindness PreventionDocument3 pagesSudha N: Retina Wellness Report For Blindness PreventionRavi ShashiNo ratings yet
- Chapter 6 Corrective LensesDocument24 pagesChapter 6 Corrective LensesSoorav MlicNo ratings yet
- Extraocular Muscles: Functions, Innervations and Motility TestingDocument62 pagesExtraocular Muscles: Functions, Innervations and Motility TestingPrincess Noreen SavellanoNo ratings yet
- Glaucoma: Pgmi Abadilla Angela MarieDocument29 pagesGlaucoma: Pgmi Abadilla Angela MarieAngel AbadillaNo ratings yet
- Postgraduate Ophthalmology Exams in IrelandDocument22 pagesPostgraduate Ophthalmology Exams in IrelandAna-Maria Misici100% (2)
- Physio B - Vision Experiment (Daenerys)Document4 pagesPhysio B - Vision Experiment (Daenerys)nva226100% (4)
- Corneoscleral T&S - PrinciplesDocument10 pagesCorneoscleral T&S - PrinciplesMuhammad SyamilNo ratings yet
- Head, Neck and BrainDocument460 pagesHead, Neck and BrainSonu Can100% (9)
- Cli&Exa&Oph&2 NDDocument420 pagesCli&Exa&Oph&2 NDPink FongNo ratings yet
- Catalogo Lentes VolkDocument48 pagesCatalogo Lentes VolkDepartamento ComercialNo ratings yet
- Cdem 19december WebDocument32 pagesCdem 19december WebRicardo Jonathan Ayala GarciaNo ratings yet
- Acuvue Price List-June 2021Document2 pagesAcuvue Price List-June 2021Anjul KumarNo ratings yet
- ICD-10 v2007Document1,097 pagesICD-10 v2007Glessica YouNo ratings yet
- Anatomy VitreousDocument6 pagesAnatomy VitreousPa Mei Lai100% (1)
- Vitreous Gel Eye Retinal Detachment OphthalmologistDocument12 pagesVitreous Gel Eye Retinal Detachment OphthalmologistLesTrechSaNo ratings yet
- Chapter 1: Introduction: 1.1 BiometricsDocument10 pagesChapter 1: Introduction: 1.1 BiometricsAnkur KumarNo ratings yet
- Biju Thankachan Thesis FinalDocument76 pagesBiju Thankachan Thesis FinalBiju ThankachanNo ratings yet
- OphthalmologyDocument5 pagesOphthalmologyGudapati Surendranadhchowdhary100% (1)
- Essential Ophthalmology NotesDocument31 pagesEssential Ophthalmology NotesHashim Ahmad50% (2)
- Ocular Manifestations of Connective Tissue Disorders: A Descriptive Cross Sectional StudyDocument4 pagesOcular Manifestations of Connective Tissue Disorders: A Descriptive Cross Sectional StudyIJAR JOURNALNo ratings yet
- Zia Chaudhury Volume - 1Document1,130 pagesZia Chaudhury Volume - 1tanya sagar0% (1)