You might also like
- Current Medications (Special Needs/Disabilities (Please Complete The Attached Individualized Care Plan Form)Document1 pageCurrent Medications (Special Needs/Disabilities (Please Complete The Attached Individualized Care Plan Form)ymcawncNo ratings yet
- 2012-2013 Corpening Memorial Center Youth Information FormDocument1 page2012-2013 Corpening Memorial Center Youth Information FormymcawncNo ratings yet
- 2012 Asheville YMCA Youth Information FormDocument1 page2012 Asheville YMCA Youth Information FormymcawncNo ratings yet
- Child's InformationDocument1 pageChild's InformationymcawncNo ratings yet
- 2013-2014 Corpening Memorial Center Youth Information FormDocument1 page2013-2014 Corpening Memorial Center Youth Information FormymcawncNo ratings yet
- 2012-2013 Corpening Memorial Branch Youth Information FormDocument1 page2012-2013 Corpening Memorial Branch Youth Information FormymcawncNo ratings yet
- 2013-2014 Corpening Memorial Center Youth Information FormDocument1 page2013-2014 Corpening Memorial Center Youth Information FormymcawncNo ratings yet
- 2013 ApplicationDocument2 pages2013 ApplicationSenseScience13No ratings yet
- StuCo Information SheetDocument2 pagesStuCo Information SheetJoshua BaconNo ratings yet
- Student Information CardDocument2 pagesStudent Information Cardptrces6494No ratings yet
- Local Membership AppDocument2 pagesLocal Membership Appapi-31215843No ratings yet
- Application Form NipDocument1 pageApplication Form Nipsyed kashif pervezNo ratings yet
- Student Information Sheet RevisedDocument1 pageStudent Information Sheet RevisedjennyNo ratings yet
- MCMA Nashville Payment FormDocument1 pageMCMA Nashville Payment FormmcmawebNo ratings yet
- Please Complete A Form For EACH Student.: Last First Middle InitialDocument4 pagesPlease Complete A Form For EACH Student.: Last First Middle InitialhwienNo ratings yet
- Worksheet in English5 Week 2 Q1Document2 pagesWorksheet in English5 Week 2 Q1Darleen VillenaNo ratings yet
- Volunteer Sign UpDocument2 pagesVolunteer Sign UpfemtchNo ratings yet
- 2012-2013 Ub Resume Fill in Format 1Document3 pages2012-2013 Ub Resume Fill in Format 1api-259154501No ratings yet
- Paper ApplicationDocument6 pagesPaper ApplicationSantosha InguvaNo ratings yet
- Emple Eth Holom: 2008/2009 Membership ApplicationDocument4 pagesEmple Eth Holom: 2008/2009 Membership ApplicationTemple Beth Sholom100% (1)
- Print MB Address2!8!2012Document2 pagesPrint MB Address2!8!2012Laura Rajsic-LanierNo ratings yet
- Coff Admission AppDocument3 pagesCoff Admission Appapi-214992453No ratings yet
- Guidance Office Personal Data InventoryDocument16 pagesGuidance Office Personal Data InventoryCharlyn May Valenzuela SimonNo ratings yet
- Registrationform 2012Document1 pageRegistrationform 2012api-205360727No ratings yet
- MMW Form IntakeformDocument1 pageMMW Form Intakeformapi-325011051No ratings yet
- Seminar Form Page 1Document2 pagesSeminar Form Page 1Fazil JafarNo ratings yet
- Membership Application 17-18Document2 pagesMembership Application 17-18api-228956733No ratings yet
- Apply For A DogDocument1 pageApply For A Dogapi-249408676No ratings yet
- WVenrollmentDocument1 pageWVenrollmentislandboyempireNo ratings yet
- Application Form: Personal InformationDocument2 pagesApplication Form: Personal InformationMuzamil HussainNo ratings yet
- Application For Admission - Middle and High School: ApplicantDocument2 pagesApplication For Admission - Middle and High School: ApplicantRafaelNo ratings yet
- Family Reunion EvaluationDocument1 pageFamily Reunion EvaluationMonique HuntNo ratings yet
- School FormsDocument2 pagesSchool FormslavariaserlinyNo ratings yet
- Applicant: For Spring 2013 or Fall 2013 EnrollmentDocument5 pagesApplicant: For Spring 2013 or Fall 2013 EnrollmentDavi SenaNo ratings yet
- Humber Extramural Registration Form 2011-2012: A. Contact InformationDocument2 pagesHumber Extramural Registration Form 2011-2012: A. Contact InformationThushanth ChandrakumarNo ratings yet
- Emergency Contact FormDocument1 pageEmergency Contact Formcernstes41No ratings yet
- CET Volunteer ApplicationDocument3 pagesCET Volunteer ApplicationRufa FernandoNo ratings yet
- Info SheetDocument1 pageInfo SheetShaun Louis AbunyawanNo ratings yet
- MCMA New York Payment FormDocument1 pageMCMA New York Payment FormmcmawebNo ratings yet
- Junior State of America Tax Form: SCHOOL NAME: - DATEDocument4 pagesJunior State of America Tax Form: SCHOOL NAME: - DATEwilliam_a_duNo ratings yet
- BCYD Membership ApplicationDocument1 pageBCYD Membership ApplicationbaycountydemsNo ratings yet
- Candidate Introduction Form: Please Affix Your Photograph HereDocument1 pageCandidate Introduction Form: Please Affix Your Photograph HeremadhursibalNo ratings yet
- Mock College App CKDocument14 pagesMock College App CKapi-545853475No ratings yet
- Sis-Form SLNHSDocument1 pageSis-Form SLNHSMICHAEL RUELONo ratings yet
- WN Volunteer Training ApplicationDocument3 pagesWN Volunteer Training ApplicationKitsilano HouseNo ratings yet
- Registration Form ScribdDocument1 pageRegistration Form ScribdMorgan May SparksNo ratings yet
- El Paso TransDocument1 pageEl Paso Transanon-407001No ratings yet
- Employment Application FormDocument5 pagesEmployment Application FormRJ Crafty InkNo ratings yet
- New Student QuestionnaireDocument2 pagesNew Student QuestionnaireMorgan ChristensenNo ratings yet
- Student Profile Form 1Document1 pageStudent Profile Form 1Angelika KlaireNo ratings yet
- Support Form RAHSDocument1 pageSupport Form RAHSremusddaNo ratings yet
- Membership FormDocument1 pageMembership Formapi-219300248No ratings yet
- Support Form RAHS 2013Document1 pageSupport Form RAHS 2013remusddaNo ratings yet
- Tenant ApplicationDocument2 pagesTenant ApplicationHoggz PhotographyNo ratings yet
- New Patient Form Johnson FinalDocument1 pageNew Patient Form Johnson Finalaharmo3No ratings yet
- AD Volunteer ApplicationDocument2 pagesAD Volunteer ApplicationPremedUSFSPNo ratings yet
- 2012 Child Care Services Branch Youth Information FormDocument5 pages2012 Child Care Services Branch Youth Information FormymcawncNo ratings yet
- GA Parishioner Grant 12-13Document1 pageGA Parishioner Grant 12-13Guardian Angels Catholic ChurchNo ratings yet
- GM Moh Nomination FormDocument1 pageGM Moh Nomination Formapi-243434486No ratings yet
- December Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageDecember Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayymcawncNo ratings yet
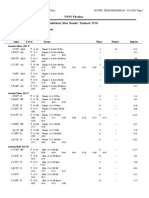
- YWNC Piranhas Individual Meet Entries ReportDocument7 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet
- YWNC Piranhas Individual Meet Entries ReportDocument3 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet
- Reuter Group Exercise: DecemberDocument1 pageReuter Group Exercise: DecemberymcawncNo ratings yet
- Time MON Tues WED Thurs FRI SAT SUN: Open GYMDocument1 pageTime MON Tues WED Thurs FRI SAT SUN: Open GYMymcawncNo ratings yet
- Fitness Class DescriptionsDocument4 pagesFitness Class DescriptionsymcawncNo ratings yet
- Base Package Base Plus PackageDocument1 pageBase Package Base Plus PackageymcawncNo ratings yet
- Ymca of Western North Carolina Afterschool Safety Plan: To Put Christian Principles Into Practice Through ProgramsDocument24 pagesYmca of Western North Carolina Afterschool Safety Plan: To Put Christian Principles Into Practice Through ProgramsymcawncNo ratings yet
- YWNC Piranhas Individual Meet Results - Standard: TUSSDocument10 pagesYWNC Piranhas Individual Meet Results - Standard: TUSSymcawncNo ratings yet
- Pool Schedule - Dec. 2013Document1 pagePool Schedule - Dec. 2013ymcawncNo ratings yet
- Do More Be More Achieve More: Lifeguard Certification CourseDocument1 pageDo More Be More Achieve More: Lifeguard Certification CourseymcawncNo ratings yet
- Ymca OF Western North Carolina: Are You Ready To Join?Document2 pagesYmca OF Western North Carolina: Are You Ready To Join?ymcawncNo ratings yet
- YWNC Piranhas Individual Meet Results - Standard: TUSSDocument9 pagesYWNC Piranhas Individual Meet Results - Standard: TUSSymcawncNo ratings yet
- NullDocument2 pagesNullymcawncNo ratings yet
- November 2013: Sun Mon Tue Wed Thu Fri SatDocument1 pageNovember 2013: Sun Mon Tue Wed Thu Fri SatymcawncNo ratings yet
- November GYM SCHEDULE: Upcoming EventsDocument1 pageNovember GYM SCHEDULE: Upcoming EventsymcawncNo ratings yet
- Asheville Group Exercise: NovemberDocument1 pageAsheville Group Exercise: NovemberymcawncNo ratings yet
- Reuter Group Exercise: NovemberDocument1 pageReuter Group Exercise: NovemberymcawncNo ratings yet
- November Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageNovember Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayymcawncNo ratings yet
- Hendersonville Group Exercise November: RM Time Class Instruc. RM Time Class Instruc. RM Time Class InstrucDocument1 pageHendersonville Group Exercise November: RM Time Class Instruc. RM Time Class Instruc. RM Time Class InstrucymcawncNo ratings yet
- October Gym Schedule: Upcoming EventsDocument1 pageOctober Gym Schedule: Upcoming EventsymcawncNo ratings yet
- YWNC Piranhas Individual Meet Entries ReportDocument4 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet
- Piranha 2013-14 Short Course Meet Schedule: RAYS-Atlanta USA 13/overs Updated 14/octDocument2 pagesPiranha 2013-14 Short Course Meet Schedule: RAYS-Atlanta USA 13/overs Updated 14/octymcawncNo ratings yet
- November 2013Document2 pagesNovember 2013ymcawncNo ratings yet
- YWNC Piranhas Individual Meet Results - Standard: TUSSDocument14 pagesYWNC Piranhas Individual Meet Results - Standard: TUSSymcawncNo ratings yet
- Do More Be More Achieve More: Lifeguard Certification CourseDocument1 pageDo More Be More Achieve More: Lifeguard Certification CourseymcawncNo ratings yet
- SKIP: Also Known As Parent/Child Is A: (Break For Thanksgiving)Document2 pagesSKIP: Also Known As Parent/Child Is A: (Break For Thanksgiving)ymcawncNo ratings yet
- Corpening YMCA Fall 2013 Under 10Document1 pageCorpening YMCA Fall 2013 Under 10ymcawncNo ratings yet
- YWNC Piranhas Individual Meet Results - Standard: TUSSDocument12 pagesYWNC Piranhas Individual Meet Results - Standard: TUSSymcawncNo ratings yet
- YWNC Piranhas Individual Meet Entries ReportDocument5 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet