You might also like
- 2012-2013 Corpening Memorial Center Youth Information FormDocument1 page2012-2013 Corpening Memorial Center Youth Information FormymcawncNo ratings yet
- Child's InformationDocument1 pageChild's InformationymcawncNo ratings yet
- 2013-2014 Corpening Memorial Center Youth Information FormDocument1 page2013-2014 Corpening Memorial Center Youth Information FormymcawncNo ratings yet
- 2012-2013 Corpening Memorial Branch Youth Information FormDocument1 page2012-2013 Corpening Memorial Branch Youth Information FormymcawncNo ratings yet
- 2012 Asheville YMCA Youth Information FormDocument1 page2012 Asheville YMCA Youth Information FormymcawncNo ratings yet
- Current Medications (Special Needs/Disabilities (Please Complete The Attached Individualized Care Plan Form)Document1 pageCurrent Medications (Special Needs/Disabilities (Please Complete The Attached Individualized Care Plan Form)ymcawncNo ratings yet
- Current Medications (Special Needs/Disabilities (Please Complete The Attached Individualized Care Plan Form)Document1 pageCurrent Medications (Special Needs/Disabilities (Please Complete The Attached Individualized Care Plan Form)ymcawncNo ratings yet
- StuCo Information SheetDocument2 pagesStuCo Information SheetJoshua BaconNo ratings yet
- Local Membership AppDocument2 pagesLocal Membership Appapi-31215843No ratings yet
- E-MailDocument2 pagesE-Mailapi-11375880No ratings yet
- 2013 ApplicationDocument2 pages2013 ApplicationSenseScience13No ratings yet
- Child's InformationDocument12 pagesChild's InformationymcawncNo ratings yet
- Dog Gone Place On-Line Application: Parent InformationDocument1 pageDog Gone Place On-Line Application: Parent InformationAlysson Lane VisnicNo ratings yet
- ApplicationDocument2 pagesApplicationGrace Deleeuw PelusoNo ratings yet
- MMW Form IntakeformDocument1 pageMMW Form Intakeformapi-325011051No ratings yet
- Apply For A DogDocument1 pageApply For A Dogapi-249408676No ratings yet
- GM Moh Nomination FormDocument1 pageGM Moh Nomination Formapi-243434486No ratings yet
- Pageant LeahDocument1 pagePageant LeahLeah A'Lisa BrownNo ratings yet
- Music Equipment Borrowing ContractDocument1 pageMusic Equipment Borrowing ContractTammy FeinbergNo ratings yet
- WN Volunteer Training ApplicationDocument3 pagesWN Volunteer Training ApplicationKitsilano HouseNo ratings yet
- AsdfasdfasdfasdfasdfaDocument1 pageAsdfasdfasdfasdfasdfaapi-317333992No ratings yet
- Sis-Form SLNHSDocument1 pageSis-Form SLNHSMICHAEL RUELONo ratings yet
- Application Form InitialDocument2 pagesApplication Form InitialSaori NagaseNo ratings yet
- GA Parishioner Grant 12-13Document1 pageGA Parishioner Grant 12-13Guardian Angels Catholic ChurchNo ratings yet
- Print MB Address2!8!2012Document2 pagesPrint MB Address2!8!2012Laura Rajsic-LanierNo ratings yet
- ApplicationDocument3 pagesApplicationapi-107554386No ratings yet
- Volunteer Sign UpDocument2 pagesVolunteer Sign UpfemtchNo ratings yet
- CULATE DESIGNS STAFF FORM NewDocument2 pagesCULATE DESIGNS STAFF FORM Newolasunkanmi hassanNo ratings yet
- Client IntakeDocument1 pageClient Intakeapi-208316567No ratings yet
- Athletic Information FormDocument5 pagesAthletic Information FormGino LudoviceNo ratings yet
- Sample Employment AppDocument2 pagesSample Employment AppjksongNo ratings yet
- Coff Admission AppDocument3 pagesCoff Admission Appapi-214992453No ratings yet
- Assignment 8Document2 pagesAssignment 8Zain MalikNo ratings yet
- Childs Information USDocument1 pageChilds Information USashishgaur007No ratings yet
- 2012 Child Care Services Branch Youth Information FormDocument5 pages2012 Child Care Services Branch Youth Information FormymcawncNo ratings yet
- Membership FormDocument1 pageMembership Formapi-219300248No ratings yet
- Mau Don Xin Viec Ngan HanDocument3 pagesMau Don Xin Viec Ngan HanalseriNo ratings yet
- RegisDocument1 pageRegisapi-245872951No ratings yet
- Change of Address Form (1)Document2 pagesChange of Address Form (1)ssimpson87935No ratings yet
- Application For Summer CampDocument1 pageApplication For Summer CampgenapeaNo ratings yet
- Guys Night Out - Permission Slip - January 2011Document1 pageGuys Night Out - Permission Slip - January 2011Pastor DwayneNo ratings yet
- Student Information CardDocument2 pagesStudent Information Cardptrces6494No ratings yet
- enrollment formDocument5 pagesenrollment formapi-738612218No ratings yet
- Children's Choir AuditionDocument1 pageChildren's Choir AuditionLiebe Ruiz TorresNo ratings yet
- Info SheetDocument1 pageInfo SheetShaun Louis AbunyawanNo ratings yet
- Shrek Emercency Contact FormDocument2 pagesShrek Emercency Contact FormChristina CannillaNo ratings yet
- Band Credit Application 2013Document2 pagesBand Credit Application 2013morrisonbrothersNo ratings yet
- Fall 2009 Youth Program Registration FormDocument1 pageFall 2009 Youth Program Registration FormchaclynknowsNo ratings yet
- 2013 Womens Spring Retreat RegistrationDocument1 page2013 Womens Spring Retreat RegistrationLauren ReisigNo ratings yet
- Patient Registraton Form - ApaDocument1 pagePatient Registraton Form - ApaYuli ParamitaNo ratings yet
- GAL Application - Become A GAL in SCDocument5 pagesGAL Application - Become A GAL in SCWylde FaerieNo ratings yet
- Emergency Contact FormDocument1 pageEmergency Contact Formcernstes41No ratings yet
- Updated-GET Global 2009 - ApplicationDocument7 pagesUpdated-GET Global 2009 - Applicationrkvance5No ratings yet
- College Scholarship AppDocument2 pagesCollege Scholarship AppfisherassistantNo ratings yet
- StudentiformationsheetDocument1 pageStudentiformationsheetapi-255720367No ratings yet
- Around The Clock Childcare LTD Enrollment Form-12rieDocument4 pagesAround The Clock Childcare LTD Enrollment Form-12rieapi-251659956No ratings yet
- Day Camp Registration Form 2013Document1 pageDay Camp Registration Form 2013api-123486123No ratings yet
- ApplicationformDocument2 pagesApplicationformapi-356718992No ratings yet
- PRC Renewal FormDocument2 pagesPRC Renewal Formiza suarezNo ratings yet
- YWNC Piranhas Individual Meet Entries ReportDocument3 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet
- YWNC Piranhas Individual Meet Entries ReportDocument7 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet
- NullDocument1 pageNullymcawncNo ratings yet
- AnnouncementsDocument1 pageAnnouncementsymcawncNo ratings yet
- December Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageDecember Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayymcawncNo ratings yet
- Ymca of Western North Carolina Afterschool Safety Plan: To Put Christian Principles Into Practice Through ProgramsDocument24 pagesYmca of Western North Carolina Afterschool Safety Plan: To Put Christian Principles Into Practice Through ProgramsymcawncNo ratings yet
- Reuter Group Exercise: DecemberDocument1 pageReuter Group Exercise: DecemberymcawncNo ratings yet
- Pool Schedule - Dec. 2013Document1 pagePool Schedule - Dec. 2013ymcawncNo ratings yet
- Corpening Group Exercise November: Monday Tuesday WednesdayDocument1 pageCorpening Group Exercise November: Monday Tuesday WednesdayymcawncNo ratings yet
- Time MON Tues WED Thurs FRI SAT SUN: Open GYMDocument1 pageTime MON Tues WED Thurs FRI SAT SUN: Open GYMymcawncNo ratings yet
- Do More Be More Achieve More: Lifeguard Certification CourseDocument1 pageDo More Be More Achieve More: Lifeguard Certification CourseymcawncNo ratings yet
- November 2013Document2 pagesNovember 2013ymcawncNo ratings yet
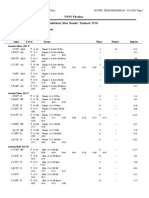
- YWNC Piranhas Individual Meet Results - Standard: TUSSDocument9 pagesYWNC Piranhas Individual Meet Results - Standard: TUSSymcawncNo ratings yet
- YWNC Piranhas Individual Meet Results - Standard: TUSSDocument10 pagesYWNC Piranhas Individual Meet Results - Standard: TUSSymcawncNo ratings yet
- Base Package Base Plus PackageDocument1 pageBase Package Base Plus PackageymcawncNo ratings yet
- Fitness Class DescriptionsDocument4 pagesFitness Class DescriptionsymcawncNo ratings yet
- Ymca OF Western North Carolina: Are You Ready To Join?Document2 pagesYmca OF Western North Carolina: Are You Ready To Join?ymcawncNo ratings yet
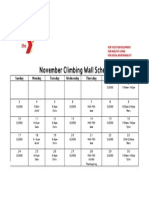
- November Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageNovember Climbing Wall Schedule: Sunday Monday Tuesday Wednesday Thursday Friday SaturdayymcawncNo ratings yet
- November GYM SCHEDULE: Upcoming EventsDocument1 pageNovember GYM SCHEDULE: Upcoming EventsymcawncNo ratings yet
- NullDocument1 pageNullymcawncNo ratings yet
- Hendersonville Group Exercise November: RM Time Class Instruc. RM Time Class Instruc. RM Time Class InstrucDocument1 pageHendersonville Group Exercise November: RM Time Class Instruc. RM Time Class Instruc. RM Time Class InstrucymcawncNo ratings yet
- NullDocument2 pagesNullymcawncNo ratings yet
- October Gym Schedule: Upcoming EventsDocument1 pageOctober Gym Schedule: Upcoming EventsymcawncNo ratings yet
- AnnouncementsDocument1 pageAnnouncementsymcawncNo ratings yet
- November 2013: Sun Mon Tue Wed Thu Fri SatDocument1 pageNovember 2013: Sun Mon Tue Wed Thu Fri SatymcawncNo ratings yet
- YWNC Piranhas Individual Meet Entries ReportDocument4 pagesYWNC Piranhas Individual Meet Entries ReportymcawncNo ratings yet
- Asheville Group Exercise: NovemberDocument1 pageAsheville Group Exercise: NovemberymcawncNo ratings yet
- NullDocument5 pagesNullymcawncNo ratings yet
- November 2013Document2 pagesNovember 2013ymcawncNo ratings yet
- Corpening Group Exercise November: Monday Tuesday WednesdayDocument1 pageCorpening Group Exercise November: Monday Tuesday WednesdayymcawncNo ratings yet