You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Physiology - Regulation of Body TemperatureDocument35 pagesPhysiology - Regulation of Body TemperatureGhaidaa Sadeq100% (2)
- Ecg NoobsDocument103 pagesEcg NoobsGhaidaa Sadeq100% (1)
- Ecg NoobsDocument103 pagesEcg NoobsGhaidaa Sadeq100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- OCR Biology F211 Cells, Exchange and Transport Revision NotesDocument4 pagesOCR Biology F211 Cells, Exchange and Transport Revision Notes24wrightphilip100% (1)
- Fatty Acid OxidationDocument46 pagesFatty Acid OxidationGhaidaa SadeqNo ratings yet
- Anatomy Upper Limb ScapulohumeraDocument48 pagesAnatomy Upper Limb ScapulohumeraGhaidaa SadeqNo ratings yet
- Embryology Cardiovascula Rsystem DevelopmentDocument128 pagesEmbryology Cardiovascula Rsystem DevelopmentGhaidaa SadeqNo ratings yet
- Fetal CirculationDocument4 pagesFetal CirculationNishaThakuriNo ratings yet
- Quick Guide To Cardiopulmonary Care 4th EditionDocument185 pagesQuick Guide To Cardiopulmonary Care 4th EditionLorenzo Romero AlbarranNo ratings yet
- Jaundice Biochemical ProfileDocument64 pagesJaundice Biochemical ProfileGhaidaa SadeqNo ratings yet
- CHF Cardiomegaly Volume OverloadDocument1 pageCHF Cardiomegaly Volume Overloadnursing concept mapsNo ratings yet
- Case Presentation - Hypovolemic ShockDocument19 pagesCase Presentation - Hypovolemic ShockIvy Jenica Mamuad50% (2)
- 1 Practise Questions Keith Moore 5th Edition Should ReadDocument113 pages1 Practise Questions Keith Moore 5th Edition Should ReadNasan Shehada100% (1)
- Part 2: Patient History: Chief ComplaintDocument11 pagesPart 2: Patient History: Chief ComplaintDavid Lim Su Shen100% (2)
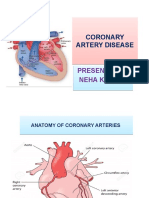
- Coronary Artery DiseaseDocument22 pagesCoronary Artery DiseaseApil BhutaniNo ratings yet
- Ophthalmology Important QuestionsDocument9 pagesOphthalmology Important QuestionsGhaidaa SadeqNo ratings yet
- The Paleo Manifesto by John Durant - ExcerptDocument17 pagesThe Paleo Manifesto by John Durant - ExcerptCrown Publishing GroupNo ratings yet
- 2nd Year Biochemistry Mnemonics PDFDocument36 pages2nd Year Biochemistry Mnemonics PDFGhaidaa SadeqNo ratings yet
- Cebu Institute of Technology - University College of NursingDocument7 pagesCebu Institute of Technology - University College of NursingGhaidaa SadeqNo ratings yet
- NetworkDocument18 pagesNetworkGhaidaa SadeqNo ratings yet
- Taking A History 1:section 1 Asking Basic Questions .: - Language Focus 1Document66 pagesTaking A History 1:section 1 Asking Basic Questions .: - Language Focus 1Ghaidaa SadeqNo ratings yet
- Physio Saq With AnswersDocument15 pagesPhysio Saq With AnswersGhaidaa SadeqNo ratings yet
- Fatty Acids SynthesisDocument30 pagesFatty Acids SynthesisGhaidaa SadeqNo ratings yet
- Anatomy of The FootDocument40 pagesAnatomy of The FootGhaidaa SadeqNo ratings yet
- Computer ConsistsDocument41 pagesComputer ConsistsGhaidaa SadeqNo ratings yet
- Adrenal Gland: by Mickey & BillyDocument23 pagesAdrenal Gland: by Mickey & BillyGhaidaa Sadeq100% (1)
- Lipid MetabolismDocument78 pagesLipid MetabolismGhaidaa SadeqNo ratings yet
- Canals, Fissures, and Foramina of Cranial Bones: Orbital RegionDocument7 pagesCanals, Fissures, and Foramina of Cranial Bones: Orbital RegionGhaidaa SadeqNo ratings yet
- Smooth Muscle Contracts Slowly and EfficientlyDocument13 pagesSmooth Muscle Contracts Slowly and EfficientlyGhaidaa SadeqNo ratings yet
- Structural Organization of The Nervous SystemDocument14 pagesStructural Organization of The Nervous SystemGhaidaa SadeqNo ratings yet
- Scalp With All DetailsDocument30 pagesScalp With All DetailsGhaidaa SadeqNo ratings yet
- Tut Physiology 2Document7 pagesTut Physiology 2Ghaidaa SadeqNo ratings yet
- Science Grade 9 LM CONTENT 1Document185 pagesScience Grade 9 LM CONTENT 1Alexes Alyza CañeteNo ratings yet
- Aortic ValveDocument8 pagesAortic ValveIfeanyichukwu OgbonnayaNo ratings yet
- Cardiac DiseasesDocument8 pagesCardiac DiseasesTJ NgNo ratings yet
- Congestive Renal FailureDocument9 pagesCongestive Renal FailureSayf QisthiNo ratings yet
- Pathology and Physiology Nums McqsDocument68 pagesPathology and Physiology Nums McqsZara100% (1)
- Dimension of Development: Health AwarenessDocument46 pagesDimension of Development: Health AwarenessBeverly TogononNo ratings yet
- Excitation of HeartDocument17 pagesExcitation of HeartdevdsantoshNo ratings yet
- Dwnload Full Holes Human Anatomy and Physiology 15th Edition Shier Solutions Manual PDFDocument35 pagesDwnload Full Holes Human Anatomy and Physiology 15th Edition Shier Solutions Manual PDFbrecciamoodgflo100% (9)
- Heart Rate MeasurementDocument15 pagesHeart Rate MeasurementK.R.Raguram100% (1)
- Hipotensi Ortostatik JurnalDocument4 pagesHipotensi Ortostatik JurnalmuhammadNo ratings yet
- Pedia NotesDocument4 pagesPedia NotesSarah Mae SilvestreNo ratings yet
- Skill 1: Main Idea QuestionsDocument6 pagesSkill 1: Main Idea QuestionsHayaaNo ratings yet
- Chapter 22 Assessment of Cardiovascualr SysteamDocument36 pagesChapter 22 Assessment of Cardiovascualr Systeamسلطان محمد فوزي سلمانNo ratings yet
- CHNDocument11 pagesCHNFranz RSNo ratings yet
- ELECTROCARDIOGRAMDocument63 pagesELECTROCARDIOGRAMMbah GapinbissiNo ratings yet
- Healthy Bodies Slide3Document11 pagesHealthy Bodies Slide3Larissa RevillaNo ratings yet
- Amiodarone and Lidocaine For The Treatment 1 1Document11 pagesAmiodarone and Lidocaine For The Treatment 1 1vanniNo ratings yet
- CTO - The Algorithms Within The Algorithm - Riley2018Document12 pagesCTO - The Algorithms Within The Algorithm - Riley2018Evandro Martins FilhoNo ratings yet
- Pediatric ECGDocument7 pagesPediatric ECGCivodarbo RimidubNo ratings yet
- DR AGUS SETIYANA Adult Congenital Heart Disease APDocument25 pagesDR AGUS SETIYANA Adult Congenital Heart Disease APryandikaNo ratings yet
- Science 6 Living Things and Their Environment Earth and Space As Reviewed by SME 1Document36 pagesScience 6 Living Things and Their Environment Earth and Space As Reviewed by SME 1Elma Ortega CamionNo ratings yet