You might also like
- Forklift Trainee HandbookDocument19 pagesForklift Trainee HandbookAdam Lilley0% (1)
- Industrial TherapyDocument29 pagesIndustrial TherapyMalu100% (1)
- MFT Written Exam HandbookDocument17 pagesMFT Written Exam HandbookSA_VialNo ratings yet
- Sprengel's ShoulderDocument21 pagesSprengel's ShoulderNahayo Xavier100% (1)
- Biomechanics 2Document150 pagesBiomechanics 2amitesh_mpthNo ratings yet
- Functional Assessment in PhysiotherapyDocument0 pagesFunctional Assessment in PhysiotherapyDibyendunarayan BidNo ratings yet
- Assessment and Management of Neurological Gaits: Dr. Purusotham Chippala, PHDDocument73 pagesAssessment and Management of Neurological Gaits: Dr. Purusotham Chippala, PHDAloysius Rodrigues0% (1)
- I. Objectives: Detailed Lesson Plan in Integrated Science 8Document11 pagesI. Objectives: Detailed Lesson Plan in Integrated Science 8Janet PagulayanNo ratings yet
- Physiotherapy Scope of Practice-Article PDFDocument3 pagesPhysiotherapy Scope of Practice-Article PDFeins_mptNo ratings yet
- Best Practices For Effective Corporate Crisis Management - A BreakDocument94 pagesBest Practices For Effective Corporate Crisis Management - A Breaksouthafrica111No ratings yet
- Community Based RehabilitationDocument30 pagesCommunity Based Rehabilitationfatima100% (1)
- Concepts and Foundations of RehabilitationDocument13 pagesConcepts and Foundations of Rehabilitationamitesh_mpthNo ratings yet
- The Role of Physiotherapy in RehabilitationDocument5 pagesThe Role of Physiotherapy in Rehabilitationari_alianiNo ratings yet
- Rood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesDocument3 pagesRood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesShekinah Gracia T. Mosquera100% (2)
- Gaston Farrell, Edith R. (Trans.) - Bachelard - Water and Dreams - An Essay On The Imagination of Matter (The Bachelard Translations) - The Pegasus Foundation (1983)Document214 pagesGaston Farrell, Edith R. (Trans.) - Bachelard - Water and Dreams - An Essay On The Imagination of Matter (The Bachelard Translations) - The Pegasus Foundation (1983)Dusan ArsovskiNo ratings yet
- The Indian Association of Physiotherapists - IAP Constitutions PDFDocument17 pagesThe Indian Association of Physiotherapists - IAP Constitutions PDFHasan Rahman100% (2)
- Roods ApproachDocument23 pagesRoods ApproachyigoNo ratings yet
- Community Based Rehabilitation PDFDocument2 pagesCommunity Based Rehabilitation PDFJoey17% (6)
- Ommunity Ased EhabilitationDocument43 pagesOmmunity Ased Ehabilitationbipinarora100% (3)
- Mindful Yoga by John Kabat-ZinnDocument12 pagesMindful Yoga by John Kabat-Zinnapi-31153366650% (2)
- Screening SensorimotorDocument29 pagesScreening Sensorimotoramitesh_mpthNo ratings yet
- (Understanding Contemporary Culture Series) Anita Brady, Tony Schirato - Understanding Judith Butler-SAGE Publications LTD (2010)Document156 pages(Understanding Contemporary Culture Series) Anita Brady, Tony Schirato - Understanding Judith Butler-SAGE Publications LTD (2010)DIEGO ALVARO RETAMOZO CASTILLO100% (1)
- Relationship LZDocument40 pagesRelationship LZRenzo Benvenuto0% (1)
- Role of Social Workers in CBRDocument16 pagesRole of Social Workers in CBRAna MikaNo ratings yet
- History ErgonomicDocument11 pagesHistory ErgonomicShiraz AhmadNo ratings yet
- Cyriax Technique: Submitted To Submitted byDocument38 pagesCyriax Technique: Submitted To Submitted byAkanksha Kulvanshi100% (2)
- OrthosisDocument112 pagesOrthosisChandan MahapatraNo ratings yet
- Dysphagia ManagementDocument21 pagesDysphagia ManagementSooraj A. O.100% (1)
- Community Based RehabilitationDocument8 pagesCommunity Based RehabilitationNaveen Kumar100% (1)
- Community-Based Rehabilitation (CBR) : By, Abhishek Verma M.Sc. NSG II YrDocument34 pagesCommunity-Based Rehabilitation (CBR) : By, Abhishek Verma M.Sc. NSG II YrAbhishek VermaNo ratings yet
- Past, Present and Future Research in PhysiotherapyDocument11 pagesPast, Present and Future Research in PhysiotherapyKiran Kumar Kalyanam100% (2)
- CH 1-Prevention PracticeDocument24 pagesCH 1-Prevention PracticeHafsa AzizNo ratings yet
- Critical Discourse Analysis PDFDocument105 pagesCritical Discourse Analysis PDFresfreak87% (31)
- Effect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly PopulationDocument6 pagesEffect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly Populationastrinila fauziNo ratings yet
- Community Based RehabilitationDocument25 pagesCommunity Based RehabilitationArun Jv50% (2)
- Infanib ScaleDocument18 pagesInfanib Scaleamitesh_mpthNo ratings yet
- History of CBRDocument15 pagesHistory of CBRkim100% (3)
- Recent Advances in PhysiotherapyFrom EverandRecent Advances in PhysiotherapyCecily PartridgeNo ratings yet
- The Guiding Principles of CBRDocument5 pagesThe Guiding Principles of CBRLadylyn BrazaNo ratings yet
- Geriatric RehabilitationDocument59 pagesGeriatric RehabilitationJuanitoCabatañaLimIIINo ratings yet
- Community Based Rehabilitation Part IDocument46 pagesCommunity Based Rehabilitation Part INabil Abd El-tawabNo ratings yet
- Carole Peterson, Allyssa McCabe (Auth.) - Developmental Psycholinguistics - Three Ways of Looking at A Child's Narrative-Springer US (1983)Document276 pagesCarole Peterson, Allyssa McCabe (Auth.) - Developmental Psycholinguistics - Three Ways of Looking at A Child's Narrative-Springer US (1983)Andrés Pérez PérezNo ratings yet
- Chapter Eight: Principles, Objectives and General Ap-Proaches Relating To Community-Based RehabilitationDocument5 pagesChapter Eight: Principles, Objectives and General Ap-Proaches Relating To Community-Based RehabilitationAnandhu GNo ratings yet
- Clinimetric Properties of Neuro-Motor AssessmentsDocument13 pagesClinimetric Properties of Neuro-Motor Assessmentsamitesh_mpthNo ratings yet
- Geriatric Rehabilitation: Prepared By: Floriza P. de Leon, PTRPDocument36 pagesGeriatric Rehabilitation: Prepared By: Floriza P. de Leon, PTRPFloriza de LeonNo ratings yet
- Management of CBRDocument72 pagesManagement of CBRtanya datt100% (1)
- Need For CBRDocument28 pagesNeed For CBRNaveen Kumar100% (1)
- Introductory BookletDocument78 pagesIntroductory BookletJena ManacsaNo ratings yet
- Community Based Rehabilitation (CBR) : ArticipationDocument6 pagesCommunity Based Rehabilitation (CBR) : ArticipationPooja YadavNo ratings yet
- CBR and Multidisciplinary Approach-Definition, Models of Multidisciplinary CBR, Recent AdvancesDocument29 pagesCBR and Multidisciplinary Approach-Definition, Models of Multidisciplinary CBR, Recent Advancesmayuri zanwar100% (1)
- District Rehabilitation CentresDocument19 pagesDistrict Rehabilitation CentresFEBIN RAJUNo ratings yet
- Extension Services and Mobile Health UnitDocument23 pagesExtension Services and Mobile Health UnitKandi IssayaNo ratings yet
- COMMUNITYDocument45 pagesCOMMUNITYAkshay BadoreNo ratings yet
- CBR Strategies (Ankita 2)Document25 pagesCBR Strategies (Ankita 2)Akshay BangadNo ratings yet
- Role of Physiotherapist in CBRDocument9 pagesRole of Physiotherapist in CBRTahsinur Rahman100% (1)
- District Disability Rehabilitation CentreDocument22 pagesDistrict Disability Rehabilitation Centreshodhganga100% (4)
- Polio Physiotherapy NotesDocument6 pagesPolio Physiotherapy NotesyigoNo ratings yet
- Presented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical TherapyDocument27 pagesPresented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical Therapysaba ramzanNo ratings yet
- BPT 3rd Year-Pt in Ortho ConditionsDocument5 pagesBPT 3rd Year-Pt in Ortho Conditionsvenkata ramakrishnaiahNo ratings yet
- Physiotherapy SyllabusDocument50 pagesPhysiotherapy SyllabusAdonis GaleosNo ratings yet
- Role of Occupational Therapists in CBRDocument16 pagesRole of Occupational Therapists in CBRFEBIN RAJU100% (1)
- Autogenic DrainageDocument26 pagesAutogenic DrainagenkarthikrajNo ratings yet
- Community and Government RoleDocument47 pagesCommunity and Government RoleBasayya Swamy100% (1)
- Community Based RehabilitationDocument34 pagesCommunity Based RehabilitationAshwathiNo ratings yet
- Functional Re-Education TrainingDocument24 pagesFunctional Re-Education Trainingtamilvanan3100% (1)
- International Classification of Impairments, Disabilities and HandicapsDocument22 pagesInternational Classification of Impairments, Disabilities and HandicapsTimoteo Timothy WilliamsNo ratings yet
- Constraint Induced Movement Therapy CIMTDocument22 pagesConstraint Induced Movement Therapy CIMTAniqa AsgharNo ratings yet
- Exercise Prescription For DisabledDocument51 pagesExercise Prescription For DisabledNaveen KumarNo ratings yet
- Motor Relearning Programme: Prepared by Mohammad Bin Afsar JanDocument11 pagesMotor Relearning Programme: Prepared by Mohammad Bin Afsar Jankashmala afzal100% (1)
- Bicipital TendonitisDocument2 pagesBicipital TendonitisJ Cheung100% (2)
- Vocational RehabilitationDocument11 pagesVocational RehabilitationSHAIK SHABEENANo ratings yet
- Prescription Principle of KAFODocument54 pagesPrescription Principle of KAFOFERYANDA UTAMI100% (1)
- Industrial HealthDocument22 pagesIndustrial HealthPraveen Kumar RNo ratings yet
- Aging RehabilitationDocument35 pagesAging RehabilitationdrsonuchawlaNo ratings yet
- Laser - 2nd BPT - 1st ClassDocument20 pagesLaser - 2nd BPT - 1st Classamitesh_mpthNo ratings yet
- Laser 2nd BPT - 2nd ClassDocument31 pagesLaser 2nd BPT - 2nd Classamitesh_mpthNo ratings yet
- Analysis of The Physiotherapy Industry - Challenges For MarketingDocument8 pagesAnalysis of The Physiotherapy Industry - Challenges For Marketingamitesh_mpthNo ratings yet
- Class-1 - Rehabilitation - What It Is.Document13 pagesClass-1 - Rehabilitation - What It Is.amitesh_mpth100% (1)
- Clinical Reasoning Strategies in PTDocument19 pagesClinical Reasoning Strategies in PTamitesh_mpthNo ratings yet
- Functional Decrements Among ElderlyDocument26 pagesFunctional Decrements Among Elderlyamitesh_mpthNo ratings yet
- Muscles Changes in Cerebral PalsyDocument21 pagesMuscles Changes in Cerebral Palsyamitesh_mpthNo ratings yet
- Pediatric Logy 2005Document287 pagesPediatric Logy 2005amitesh_mpthNo ratings yet
- ACT As A FadDocument22 pagesACT As A FadYusinta MuawanahNo ratings yet
- Design Department Proposal With BDes For CommentsDocument85 pagesDesign Department Proposal With BDes For CommentsfhreankNo ratings yet
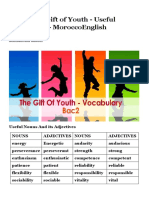
- Bac2 The Gift of Youth - Useful Vocabulary - MoroccoEnglishDocument4 pagesBac2 The Gift of Youth - Useful Vocabulary - MoroccoEnglishWalaa WalaaNo ratings yet
- Pseudonym-Lesson 4 - Multiplication Into DivisionDocument4 pagesPseudonym-Lesson 4 - Multiplication Into Divisionapi-245860433No ratings yet
- Teraphy ArtDocument10 pagesTeraphy ArtSalma ChairaniNo ratings yet
- Glued To Your Phone Generation Z's Smartphone Addiction and Online Compulsive BuyingDocument13 pagesGlued To Your Phone Generation Z's Smartphone Addiction and Online Compulsive BuyingTitaccia GianinaNo ratings yet
- Power and PoliticsDocument19 pagesPower and PoliticsNoorulainNo ratings yet
- Counseling Skills Analysis of CounselorsDocument13 pagesCounseling Skills Analysis of CounselorsPeeto PandaNo ratings yet
- SO Upper Intermediate Teacher's BookDocument98 pagesSO Upper Intermediate Teacher's BookAynur HüseynovaNo ratings yet
- Cambridge English - Key (KET) For Schools Exam Format - ListeningDocument3 pagesCambridge English - Key (KET) For Schools Exam Format - ListeningNoor AsilatiNo ratings yet
- Lesson Plan Parts-And-Total Number Stories 1Document6 pagesLesson Plan Parts-And-Total Number Stories 1api-644964217No ratings yet
- Trick QuestionDocument69 pagesTrick Questionphamlinh_cnn7625No ratings yet
- DebateDocument10 pagesDebateShayne AbellaNo ratings yet
- Comprehensive Classroom Management PlanDocument2 pagesComprehensive Classroom Management Planapi-315973172No ratings yet
- Literature Final BookDocument83 pagesLiterature Final BookKabir100% (1)
- Gopi EnglishDocument31 pagesGopi EnglishGopi ShankarNo ratings yet
- UWCiM Buzz Jan 2011Document10 pagesUWCiM Buzz Jan 2011Paul LauNo ratings yet
- CORE 001 3rd Quarter - Lesson 3Document7 pagesCORE 001 3rd Quarter - Lesson 3NatsumiGraceNo ratings yet
- Behaviorism: By: Svend Waltman For: Dr. Ann Nauman EDF 607 May, 2003Document11 pagesBehaviorism: By: Svend Waltman For: Dr. Ann Nauman EDF 607 May, 2003Yuriatson JubhariNo ratings yet
- Ultimate Ap Exam Review Part 1Document160 pagesUltimate Ap Exam Review Part 1api-287575009No ratings yet