You might also like
- 3-Electronic Health RecordDocument11 pages3-Electronic Health RecordConger Conger100% (1)
- Healthcare Environmental Services A Complete Guide - 2020 EditionFrom EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNo ratings yet
- Health Information SystemsDocument10 pagesHealth Information Systemsalexandercecilia67100% (1)
- Hospital Information Management PDFDocument192 pagesHospital Information Management PDFDhrienNo ratings yet
- Patient Safety Organization A Complete Guide - 2020 EditionFrom EverandPatient Safety Organization A Complete Guide - 2020 EditionNo ratings yet
- Payment in Healthcare OrganizationsDocument12 pagesPayment in Healthcare Organizationsevans kirimiNo ratings yet
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- Healthcare Delivery Organization CIOs A Complete Guide - 2019 EditionFrom EverandHealthcare Delivery Organization CIOs A Complete Guide - 2019 EditionNo ratings yet
- Leadership in Healthcare: Essential Values and Skills, Fourth EditionFrom EverandLeadership in Healthcare: Essential Values and Skills, Fourth EditionNo ratings yet
- Health Information TechnologyfinalDocument8 pagesHealth Information TechnologyfinalFranzia Izandra Alkuino Mojica100% (1)
- Healthcare Information System A Complete Guide - 2020 EditionFrom EverandHealthcare Information System A Complete Guide - 2020 EditionNo ratings yet
- Customer Satisfaction and Service MarketingDocument22 pagesCustomer Satisfaction and Service MarketingAnshita GargNo ratings yet
- Modern Healthcare: How Can Digital Tools Help Improve Our Overall HealthFrom EverandModern Healthcare: How Can Digital Tools Help Improve Our Overall HealthNo ratings yet
- Measuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsFrom EverandMeasuring Quality Improvement in Healthcare: A Guide to Statistical Process Control ApplicationsNo ratings yet
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipFrom EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo ratings yet
- The New Era of Regulatory Enforcement: A Comprehensive Guide for Raising the Bar to Manage RiskFrom EverandThe New Era of Regulatory Enforcement: A Comprehensive Guide for Raising the Bar to Manage RiskNo ratings yet
- Textbook of Urgent Care Management: Chapter 12, Pro Forma Financial StatementsFrom EverandTextbook of Urgent Care Management: Chapter 12, Pro Forma Financial StatementsNo ratings yet
- Mobile App Survey ReportDocument18 pagesMobile App Survey ReportvictrrocksNo ratings yet
- Medical Center Marketing PlanDocument8 pagesMedical Center Marketing PlanIan CastroNo ratings yet
- Differences between Health Informatics and Health Information ManagementDocument3 pagesDifferences between Health Informatics and Health Information ManagementDavid MeléndezNo ratings yet
- Critical Analysis of Patient and Family Rights in Jci Accreditation and Cbahi Standards For HospitalsDocument10 pagesCritical Analysis of Patient and Family Rights in Jci Accreditation and Cbahi Standards For HospitalsImpact JournalsNo ratings yet
- Healthcare IndustryDocument5 pagesHealthcare IndustryTanya ChaudharyNo ratings yet
- Hospitals and EconomicsDocument27 pagesHospitals and EconomicsUnivsan Agustin EmployeesunionNo ratings yet
- Indus HospitalDocument33 pagesIndus HospitalKhushbakht Suhail100% (1)
- Hospital Administration: Hariharan.P MSWDocument25 pagesHospital Administration: Hariharan.P MSWhariharanhrNo ratings yet
- Health Care (Hospital) Industry: Pristine HospitalsDocument27 pagesHealth Care (Hospital) Industry: Pristine Hospitalssamknight2009No ratings yet
- 5 Tips To Improve A Hospital's Brand: TagsDocument2 pages5 Tips To Improve A Hospital's Brand: Tagssaeed_alem_mec84No ratings yet
- H C I M U: Ealth ARE Ndustry Arket PdateDocument24 pagesH C I M U: Ealth ARE Ndustry Arket PdateRavi RanjanNo ratings yet
- Financing and Delivery of Health Services NCMCHDocument320 pagesFinancing and Delivery of Health Services NCMCHBrand SynapseNo ratings yet
- Cost-Effective Urgent Care Center Reduces ED OveruseDocument6 pagesCost-Effective Urgent Care Center Reduces ED Overusedaron_vchulekNo ratings yet
- Term Paper ON Hospital ManagementDocument21 pagesTerm Paper ON Hospital ManagementVandy CoolNo ratings yet
- Strengthen Patient Experience: (Implementation Plan of IDC Program) Domain 1: CommunicationDocument23 pagesStrengthen Patient Experience: (Implementation Plan of IDC Program) Domain 1: CommunicationRina LestariNo ratings yet
- Course OutlineDocument4 pagesCourse Outlineapi-382689726No ratings yet
- Nursing Home AdministratorDocument2 pagesNursing Home Administratorapi-78009605100% (1)
- Individual Project Updated VersionDocument2 pagesIndividual Project Updated VersionsherifNo ratings yet
- Healthcare Fraud Paper 1Document9 pagesHealthcare Fraud Paper 1api-609705358No ratings yet
- Joint Commission Patient-Centered Communication Standards 2011Document4 pagesJoint Commission Patient-Centered Communication Standards 2011Institute of CaliforniaNo ratings yet
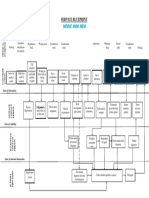
- Service Blueprint Medical CenterDocument1 pageService Blueprint Medical CenterNguyen Le Hoang KimNo ratings yet
- Introduction To Health Insurance PPT 8 23 13 FinalDocument38 pagesIntroduction To Health Insurance PPT 8 23 13 Finalapi-225367524100% (1)
- Patient Satisfaction With Primary Healthcare in Kashmir IndiaDocument12 pagesPatient Satisfaction With Primary Healthcare in Kashmir IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Business PlanDocument55 pagesBusiness PlanRabindra Raj Bista100% (1)
- HIMSS10 GuideDocument24 pagesHIMSS10 Guidemr_histalk5532No ratings yet
- @@assessment of Medical Documentation As Per Joint Commission InternationDocument6 pages@@assessment of Medical Documentation As Per Joint Commission InternationNahari ArifinNo ratings yet
- CDH Health Project CharterDocument14 pagesCDH Health Project Charterjasonkerr7No ratings yet
- Hospital PricingDocument41 pagesHospital Pricingaarti HingeNo ratings yet
- ACHC - Standards - Community RetailDocument71 pagesACHC - Standards - Community RetailServesh Tiwari100% (2)
- Online Hospital Management SystemDocument2 pagesOnline Hospital Management Systemyay guruNo ratings yet
- Healthcare Practice Office Manager in New York NY Resume Milean CasianoDocument2 pagesHealthcare Practice Office Manager in New York NY Resume Milean CasianoMileanCasiano100% (1)
- Ways To Improve The Health SystemDocument18 pagesWays To Improve The Health SystemB I N SNo ratings yet
- 8Document11 pages8Teemara King100% (1)
- Challenges To ManagersDocument1 pageChallenges To ManagersAVRajan69No ratings yet
- Cue Sheet Day-31, 14th May, 2020Document3 pagesCue Sheet Day-31, 14th May, 2020Ajlan AliNo ratings yet
- Student PerformanceDocument3 pagesStudent PerformanceAjlan AliNo ratings yet
- Medical Officer 19J2019 PDFDocument54 pagesMedical Officer 19J2019 PDFAjlan AliNo ratings yet
- Challenges To ManagersDocument1 pageChallenges To ManagersAVRajan69No ratings yet
- Patient Satisfaction Key to Quality HealthcareDocument8 pagesPatient Satisfaction Key to Quality HealthcareAjlan AliNo ratings yet
- Ramzan CalendarDocument2 pagesRamzan CalendarAjlan AliNo ratings yet
- 6.bliss House PDFDocument1 page6.bliss House PDFAjlan AliNo ratings yet
- Patient SatisfactionDocument8 pagesPatient SatisfactionAjlan AliNo ratings yet
- Patient Satisfaction Key to Quality HealthcareDocument8 pagesPatient Satisfaction Key to Quality HealthcareAjlan AliNo ratings yet
- Patient Satisfaction Key to Quality HealthcareDocument8 pagesPatient Satisfaction Key to Quality HealthcareAjlan AliNo ratings yet
- Patient Satisfaction2Document4 pagesPatient Satisfaction2Ajlan AliNo ratings yet
- Patient SatisfactionDocument8 pagesPatient SatisfactionAjlan AliNo ratings yet
- Patient SatisfactionDocument8 pagesPatient SatisfactionAjlan AliNo ratings yet
- Patient SatisfactionDocument8 pagesPatient SatisfactionAjlan AliNo ratings yet
- Patient Satisfaction2Document4 pagesPatient Satisfaction2Ajlan AliNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Clinical Anatomy by Regions' by Richard S. Snell: Book ReviewDocument1 pageClinical Anatomy by Regions' by Richard S. Snell: Book ReviewAjlan AliNo ratings yet
- Data Table CarbonDocument2 pagesData Table Carbonyodaswarrior33% (15)
- Logix5000 Control Systems: Connect Kinetix 350 Drives Over An Ethernet/Ip NetworkDocument50 pagesLogix5000 Control Systems: Connect Kinetix 350 Drives Over An Ethernet/Ip NetworkAlan Ruiz CortezNo ratings yet
- Proportional Valves: Adjustment ProcedureDocument11 pagesProportional Valves: Adjustment Procedureyaniprasetyo12No ratings yet
- Teaser Rheosolve D 15ASDocument2 pagesTeaser Rheosolve D 15ASwahyuni raufianiNo ratings yet
- Lanco Solar EPC leaderDocument19 pagesLanco Solar EPC leaderShabir TrambooNo ratings yet
- Review of Guyana's Social Education ProgramDocument6 pagesReview of Guyana's Social Education ProgramTineka Jagan CharlesNo ratings yet
- ERA News Mar 23 - Final - 0Document10 pagesERA News Mar 23 - Final - 0Băltoiu Son AlisaNo ratings yet
- Travel directions LPU-Batangas from Manila, Laguna, Quezon, CaviteDocument1 pageTravel directions LPU-Batangas from Manila, Laguna, Quezon, CaviteMark Levin Munar100% (1)
- COT English 3rd PrepositionDocument14 pagesCOT English 3rd PrepositionGanie Mae Talde Casuncad100% (1)
- DL1 - Epicyclic Gear Train & Holding Torque ManualDocument4 pagesDL1 - Epicyclic Gear Train & Holding Torque Manualer_arun76100% (1)
- # Micro Pelton Turbines ! $Document93 pages# Micro Pelton Turbines ! $Nathaniel E. Barrios Fuentes100% (1)
- 1 National Workshop For Sustainable Built Environment South - South PartnershipDocument14 pages1 National Workshop For Sustainable Built Environment South - South PartnershipRajendra KunwarNo ratings yet
- Economics Not An Evolutionary ScienceDocument17 pagesEconomics Not An Evolutionary SciencemariorossiNo ratings yet
- A Is Called The Base and N Is Called The Exponent: Grade 7 Math Lesson 21: Laws of Exponents Learning GuideDocument4 pagesA Is Called The Base and N Is Called The Exponent: Grade 7 Math Lesson 21: Laws of Exponents Learning GuideKez MaxNo ratings yet
- 3 6 17weekly Homework Sheet Week 23 - 5th Grade - CcssDocument3 pages3 6 17weekly Homework Sheet Week 23 - 5th Grade - Ccssapi-328344919No ratings yet
- Sophiajurgens Resume EdtDocument2 pagesSophiajurgens Resume Edtapi-506489381No ratings yet
- D Series: Instruction ManualDocument2 pagesD Series: Instruction ManualMartin del ValleNo ratings yet
- RV RVR en 0714 Edit PDFDocument6 pagesRV RVR en 0714 Edit PDFJacques FerreiraNo ratings yet
- Nanowires - Fundamental ResearchDocument564 pagesNanowires - Fundamental ResearchJosé Ramírez100% (1)
- August Morning WorkDocument20 pagesAugust Morning Workapi-471325484No ratings yet
- Lesson Plan SETS 2 PDFDocument10 pagesLesson Plan SETS 2 PDFHelmi Tarmizi83% (6)
- Essential Science Concepts and Laboratory ToolsDocument5 pagesEssential Science Concepts and Laboratory ToolsCathee LeañoNo ratings yet
- ASM Product Opportunity Spreadsheet2Document48 pagesASM Product Opportunity Spreadsheet2Yash SNo ratings yet
- 2013 Sunchaser Brochure PDFDocument12 pages2013 Sunchaser Brochure PDFKelly SimpsonNo ratings yet
- Hve r13Document1 pageHve r13aleem_201sNo ratings yet
- Chapter 5Document31 pagesChapter 5Marvin VinasNo ratings yet
- Advanced Long Range Proximity Reader PDFDocument1 pageAdvanced Long Range Proximity Reader PDFPhangkie RecolizadoNo ratings yet
- Engine Parts Location GuideDocument4 pagesEngine Parts Location GuidevarenziaNo ratings yet
- Cryptography and Network Security": Sir Syed University of Engineering & TechnologyDocument5 pagesCryptography and Network Security": Sir Syed University of Engineering & TechnologySehar KhanNo ratings yet
- The World in Which We Believe in Is The Only World We Live inDocument26 pagesThe World in Which We Believe in Is The Only World We Live inYusufMiddeyNo ratings yet