You might also like
- NCP ConstipationDocument3 pagesNCP ConstipationNkk Aqnd Mgdngl100% (4)
- 12 Weeks To Your Hottest Body EverDocument49 pages12 Weeks To Your Hottest Body EverSixp8ck100% (1)
- 4 EsophagealSpasm BajaDocument6 pages4 EsophagealSpasm Bajakint manlangitNo ratings yet
- Th Đề này gồm 4 trang: best answers the questionDocument4 pagesTh Đề này gồm 4 trang: best answers the questionWilliam Phoenix67% (6)
- A Case PresentationDocument50 pagesA Case PresentationAnaleah MalayaoNo ratings yet
- Hyperthermia (Thurs)Document1 pageHyperthermia (Thurs)Christine Esguerra OrozcoNo ratings yet
- NCP (Age)Document5 pagesNCP (Age)justinmhayNo ratings yet
- Nursing Care Plan - Using NandaDocument16 pagesNursing Care Plan - Using NandaWardinatul ImanNo ratings yet
- Why Vegan PDFDocument12 pagesWhy Vegan PDFanimall0ver100% (1)
- Nursing Care Plan For Acute Pancreatitis NCPDocument2 pagesNursing Care Plan For Acute Pancreatitis NCPderic89% (18)
- Ineffective Breathing PatternDocument7 pagesIneffective Breathing PatternJanmae JivNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationgabbyNo ratings yet
- Careplan Acute PancreatitisDocument2 pagesCareplan Acute PancreatitisBSN 2014100% (4)
- NCP EmphysemaDocument9 pagesNCP Emphysemahermesdave188% (8)
- NCPDocument2 pagesNCPJamaica SaranquinNo ratings yet
- Word Ncp.......... TetanusDocument6 pagesWord Ncp.......... TetanusaianrNo ratings yet
- NCPDocument2 pagesNCPNaidin Catherine De Guzman-AlcalaNo ratings yet
- Lesson Plan On HyperlipidemiaDocument4 pagesLesson Plan On HyperlipidemiaBinita Shakya100% (1)
- NCPDocument2 pagesNCPCamille VirayNo ratings yet
- NCPDocument2 pagesNCPShubhangi SarwanNo ratings yet
- Nursing Care PlanDocument20 pagesNursing Care PlanZamranosNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanDewi PurnamasariNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiNo ratings yet
- HTP Ineffective BreathingDocument3 pagesHTP Ineffective BreathingShyrra Edades PinderNo ratings yet
- HypophysectomyDocument19 pagesHypophysectomyjoel david knda mj100% (1)
- NCP - NewbornDocument1 pageNCP - NewbornChristine Michelle A. BalancadNo ratings yet
- Tonsilitis NCPDocument2 pagesTonsilitis NCPFATIMA MARYAMA USMANNo ratings yet
- Research ProposalDocument22 pagesResearch ProposalKapil LakhwaraNo ratings yet
- Fluorosis: Fluoride Toxicity: Patient Management & MonitoringDocument24 pagesFluorosis: Fluoride Toxicity: Patient Management & MonitoringdrjriNo ratings yet
- Decreased Cardiac OutputDocument4 pagesDecreased Cardiac OutputAdnan Khan100% (1)
- Drug-Study NCPDocument5 pagesDrug-Study NCPMURILLO, FRANK JOMARI C.No ratings yet
- NCPDocument3 pagesNCPJerome Vergel RubianesNo ratings yet
- Nursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToDocument1 pageNursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToVoid LessNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Word Ncp.......... TetanusDocument3 pagesWord Ncp.......... TetanusYvounne Ananias Bautista RNNo ratings yet
- Healthcare - Nursing Care Plan - Excess Fluid VolumeDocument4 pagesHealthcare - Nursing Care Plan - Excess Fluid VolumeBenjamin CañalitaNo ratings yet
- Nursing Care PlansDocument7 pagesNursing Care PlansJayson Sumampong100% (1)
- DHF NCP 2Document1 pageDHF NCP 2mavefigNo ratings yet
- Cues Nursing Diagnosis Rationale Goals and Objectives Nursing Intervention Rationale Evaluation SubjectiveDocument4 pagesCues Nursing Diagnosis Rationale Goals and Objectives Nursing Intervention Rationale Evaluation SubjectiveFaye Dianne Damian-BuenafeNo ratings yet
- Assessment Diagnosis Rationale Planning Implementation Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Implementation Rationale Evaluationkristel_nicole18yahoNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainNathalie kate petallarNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute Painmanoelsterg50% (2)
- NCPDocument15 pagesNCPCamille PinedaNo ratings yet
- Flail Chest (Tayug)Document25 pagesFlail Chest (Tayug)Adrian MallarNo ratings yet
- Nursing Care Plan Rheumatoid ArthritisDocument3 pagesNursing Care Plan Rheumatoid ArthritisJashAnia MarIe EvArdo FloresNo ratings yet
- Nursing Care Plan Peptic UlcerDocument3 pagesNursing Care Plan Peptic UlcerJefferson Baluyot PalmaNo ratings yet
- Subjective:: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesSubjective:: Assessment Diagnosis Planning Implementation Rationale EvaluationAyra PunzalanNo ratings yet
- Imbalnce Nutrition Less Than Body RequirementsDocument3 pagesImbalnce Nutrition Less Than Body RequirementselheezaNo ratings yet
- Nursing Measures To Maintain Normal Respiratory Function and OxygenationDocument2 pagesNursing Measures To Maintain Normal Respiratory Function and Oxygenationlodeth100% (2)
- Introduction To Community Health and Environmental Sanitation PDFDocument44 pagesIntroduction To Community Health and Environmental Sanitation PDFKaty SanchezNo ratings yet
- NCP (Or) ThyroidectomyDocument3 pagesNCP (Or) ThyroidectomyChiz CorreNo ratings yet
- Nursing Care PlansDocument4 pagesNursing Care Plansapi-19762967No ratings yet
- Common Nursing Diagnosis Found in Nursing Care Plans For HypertensionDocument2 pagesCommon Nursing Diagnosis Found in Nursing Care Plans For HypertensionRaveen mayiNo ratings yet
- NCP Klippel Trenaunay SyndromeDocument3 pagesNCP Klippel Trenaunay SyndromePaola Marie VenusNo ratings yet
- PeritonitisDocument6 pagesPeritonitisDiane ArgoteNo ratings yet
- Oxygen Terapi Dan PrinsipelDocument16 pagesOxygen Terapi Dan PrinsipelAmrita KaurNo ratings yet
- NCP Urine RetentionDocument4 pagesNCP Urine RetentionKingJayson Pacman06No ratings yet
- Ineffective Airway ClearanceDocument6 pagesIneffective Airway ClearanceBenly Grace Rebuyon MosquedaNo ratings yet
- NCP Risk For InfecctionDocument2 pagesNCP Risk For Infecctionsnay axieNo ratings yet
- NCM 116 - RLE Activity#1 - VALDEZ PDFDocument6 pagesNCM 116 - RLE Activity#1 - VALDEZ PDFDexel Lorren ValdezNo ratings yet
- Acute PancreatitisDocument2 pagesAcute PancreatitisAkocmeme Sanchez100% (1)
- Git Diseases OralrevDocument30 pagesGit Diseases OralrevRafi AcostaNo ratings yet
- DIVERTICULOSISDocument21 pagesDIVERTICULOSISTiffany AdriasNo ratings yet
- Dissertation Topics of PG Degree Mdms Submitted For The Academic Year 2018-19-2019 20 and 2020 21Document227 pagesDissertation Topics of PG Degree Mdms Submitted For The Academic Year 2018-19-2019 20 and 2020 21Asra QuadriNo ratings yet
- Biological EspionageDocument3 pagesBiological EspionageSasiii SoniiiNo ratings yet
- 08 16Document116 pages08 16WoodsNo ratings yet
- Genetic EngineeringDocument43 pagesGenetic EngineeringGeonyzl L. AlviolaNo ratings yet
- Marketing Safe WaterDocument120 pagesMarketing Safe WaterSTBM IndonesiaNo ratings yet
- Exceptionalities QuizDocument7 pagesExceptionalities QuizPatrick HernandezNo ratings yet
- Maternal and Child ReviewerDocument19 pagesMaternal and Child ReviewerMYKA ESPERILANo ratings yet
- Tankersley Memo Pretrial Rel Bail ReformDocument37 pagesTankersley Memo Pretrial Rel Bail ReformCLDC_GSNo ratings yet
- MainDocument3 pagesMaindivyanshu kumarNo ratings yet
- All About Rabies Health ScienceDocument28 pagesAll About Rabies Health SciencetototoNo ratings yet
- Scale For Ranking Family Health Problems Accdg To PrioritiesDocument3 pagesScale For Ranking Family Health Problems Accdg To PrioritiesArthur Brian Panit100% (1)
- Ekg PJKDocument110 pagesEkg PJKDexel Putra SimbolonNo ratings yet
- Excerpt From Apollo's Arrow: The Profound and Enduring Impact of Coronavirus On The Way We Live" by Nicholas ChristakisDocument4 pagesExcerpt From Apollo's Arrow: The Profound and Enduring Impact of Coronavirus On The Way We Live" by Nicholas ChristakisOnPointRadioNo ratings yet
- Aw-14517-001 003 01Document104 pagesAw-14517-001 003 01Maldwin MenorcaNo ratings yet
- Antenatal CareDocument29 pagesAntenatal Careعبدالكريم الاسدNo ratings yet
- Gene Therapy: Laguna State Polytechnic University San Pablo CityDocument11 pagesGene Therapy: Laguna State Polytechnic University San Pablo CityAndromeda GalaxyNo ratings yet
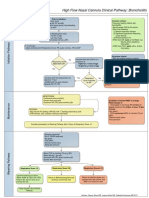
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- Naskah PublikasiDocument10 pagesNaskah PublikasiSarah Certainly' CleverNo ratings yet
- English NotesDocument30 pagesEnglish NotesJose Payne50% (4)
- MicrosatellitesDocument24 pagesMicrosatellitesAhmed BioNo ratings yet
- Medical Case 3: Vincent Brody: Guided Reflection QuestionsDocument3 pagesMedical Case 3: Vincent Brody: Guided Reflection Questionsapi-546220765No ratings yet
- Med Surg 1Document26 pagesMed Surg 1RogerQuxNo ratings yet
- Product Hygiene Issues and Its Impact On Consumer's Buying Pattern and Product Sales A Case Study of Dairy Tetra Pack Versus Open Market ProductDocument81 pagesProduct Hygiene Issues and Its Impact On Consumer's Buying Pattern and Product Sales A Case Study of Dairy Tetra Pack Versus Open Market ProductRehan RaufNo ratings yet
- Visual Impairment ScriptDocument3 pagesVisual Impairment Scriptapi-285548719No ratings yet
- Fresh Air Camp Application 2010Document13 pagesFresh Air Camp Application 2010Morgan Memorial Goodwill IndustriesNo ratings yet
- Rationale and Evidence ICDAS II September 11-1 PDFDocument43 pagesRationale and Evidence ICDAS II September 11-1 PDFmahmoudNo ratings yet