
You might also like
- Learning Plan Nursing PregradDocument3 pagesLearning Plan Nursing Pregradapi-25180064033% (3)
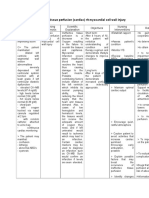
- Nursing Diagnosis Diabetic KetoacidosisDocument11 pagesNursing Diagnosis Diabetic Ketoacidosismonisha50% (4)
- Acute Coronary Syndrome NCP 02Document6 pagesAcute Coronary Syndrome NCP 02AgronaSlaughterNo ratings yet
- Acute Coronary Syndrome NCP 01Document5 pagesAcute Coronary Syndrome NCP 01AgronaSlaughter0% (1)
- Coronary Artery Disease Care PlanDocument2 pagesCoronary Artery Disease Care PlanDanelle Harrison, RN100% (2)
- Controlling Microbial Growth in VitroDocument65 pagesControlling Microbial Growth in VitroCarl Elexer Cuyugan Ano100% (16)
- NCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNDocument1 pageNCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNCarl Elexer Cuyugan Ano100% (2)
- NCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNDocument1 pageNCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNCarl Elexer Cuyugan Ano100% (2)
- Healthcare - Nursing Care Plan - Decreased Cardiac OutputDocument4 pagesHealthcare - Nursing Care Plan - Decreased Cardiac OutputBenjamin CañalitaNo ratings yet
- NCP. Decreased Cardiac OutputDocument5 pagesNCP. Decreased Cardiac OutputJillian AmponinNo ratings yet
- Care Plan Unstable AnginaDocument4 pagesCare Plan Unstable Anginaالغزال الذهبي50% (6)
- NCP AnginaDocument3 pagesNCP AnginaShie LA100% (1)
- NURSING CARE PLAN For Myocardial InfarctionDocument16 pagesNURSING CARE PLAN For Myocardial InfarctionFreisanChenMandumotan100% (1)
- Nursing Care Plan For A Patient With Pleural EffusionDocument5 pagesNursing Care Plan For A Patient With Pleural Effusionmac042250% (4)
- Myocarditis NCP 2Document8 pagesMyocarditis NCP 2astro_aaron117375% (4)
- Buergers Disease NCPDocument5 pagesBuergers Disease NCPNikko Dela Cruz100% (2)
- Activity Intolerance Related To Decrease Blood FlowDocument3 pagesActivity Intolerance Related To Decrease Blood FlowDarkCeades100% (3)
- SAMPLE NCP For Angina PectorisDocument3 pagesSAMPLE NCP For Angina Pectorisseanne_may100% (4)
- NCP (Icu)Document2 pagesNCP (Icu)jessie_nuñez_263% (8)
- Family Case Analysis 2Document98 pagesFamily Case Analysis 2Carl Elexer Cuyugan Ano50% (2)
- PainDocument44 pagesPainCarl Elexer Cuyugan Ano100% (4)
- NCP - Risk For Impaired Skin Integrity R/T Dry Skin and Behaviors That May Lead To Skin Integrity Impairment AEB Scratching of ScabsDocument1 pageNCP - Risk For Impaired Skin Integrity R/T Dry Skin and Behaviors That May Lead To Skin Integrity Impairment AEB Scratching of ScabsCarl Elexer Cuyugan Ano100% (4)
- Seminar InsightsDocument2 pagesSeminar InsightsMark Lorenzo Torres67% (6)
- NCP For Acute Coronary SyndromeDocument3 pagesNCP For Acute Coronary Syndromesarahtot75% (4)
- NCP For SVTDocument6 pagesNCP For SVTRen VillenaNo ratings yet
- NCP For AnginaDocument5 pagesNCP For Anginacarizza_bernas100% (1)
- Nursing Care PlanDocument7 pagesNursing Care PlanGem Ma100% (7)
- NCP FVDDocument2 pagesNCP FVDMarlon AnryNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationChristine LebicoNo ratings yet
- Nursing Care Plan For A Patient With Pleural EffusionDocument4 pagesNursing Care Plan For A Patient With Pleural EffusionTrixie Anne GamotinNo ratings yet
- NCPDocument4 pagesNCPElbert Vierneza100% (2)
- Nanda NCP BasedDocument14 pagesNanda NCP Baseddeliejoyce100% (1)
- NCP - Excess Fluid Volume (Aortic Stenosis)Document3 pagesNCP - Excess Fluid Volume (Aortic Stenosis)Daniel Vergara Arce100% (3)
- NCP Impaired Gas Exhange CHEST INJURYDocument4 pagesNCP Impaired Gas Exhange CHEST INJURYMa. Elaine Carla Tating100% (2)
- Decreased Cardiac OutputDocument2 pagesDecreased Cardiac OutputEdrianne J.100% (2)
- NCP 1Document1 pageNCP 1hsiriaNo ratings yet
- Dka NCPDocument3 pagesDka NCPMaryjoy Gabriellee De La CruzNo ratings yet
- NCP Heart BlockDocument3 pagesNCP Heart BlockEköw Santiago Javier33% (3)
- NCP Pleural EffusionDocument3 pagesNCP Pleural EffusionEli Xma100% (1)
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- NCP Inffective Tissue PerfusionDocument3 pagesNCP Inffective Tissue PerfusionPaul Cubacub0% (1)
- Nursing Care Plan (NCP) For A Patient With Angina PectorisDocument3 pagesNursing Care Plan (NCP) For A Patient With Angina PectorisKian Herrera100% (1)
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanShiella Heart MalanaNo ratings yet
- Myocardial InfarctionDocument5 pagesMyocardial InfarctionDharline Abbygale Garvida AgullanaNo ratings yet
- Risk For Decreased Cardiac OutputDocument3 pagesRisk For Decreased Cardiac OutputSid Artemis FriasNo ratings yet
- NCPDocument7 pagesNCPChris Denver BancaleNo ratings yet
- NCPDocument7 pagesNCPJo Chiko FlorendoNo ratings yet
- Uti NCPDocument1 pageUti NCPAngelique Vinoya100% (2)
- Decrease Cardiac OutputDocument6 pagesDecrease Cardiac OutputGerardeanne ReposarNo ratings yet
- NCPDocument4 pagesNCPRachel PerandoNo ratings yet
- NCP - Risk For Infection - DMDocument3 pagesNCP - Risk For Infection - DMcessi18100% (1)
- NURSING CARE PLAN Decreased Cardiac Output FnaDocument2 pagesNURSING CARE PLAN Decreased Cardiac Output FnaAce Dioso Tubasco100% (1)
- NCP For CTTDocument1 pageNCP For CTTJen Rhae LimNo ratings yet
- NCP For Mi PainDocument2 pagesNCP For Mi PainKahMallariNo ratings yet
- Decreased Cardiac OutputDocument2 pagesDecreased Cardiac OutputDheza Rodis Santos0% (1)
- NCPDocument15 pagesNCPCamille PinedaNo ratings yet
- Nursing Care Plan: Subjective DataDocument4 pagesNursing Care Plan: Subjective DataAbdallah AlasalNo ratings yet
- NURSING CARE PLAN - Myocardial Infarction Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument4 pagesNURSING CARE PLAN - Myocardial Infarction Assessment Diagnosis Inference Planning Intervention Rationale Evaluationsweethoney220% (1)
- NCP AneurysmDocument4 pagesNCP AneurysmJanielle Christine Monsalud100% (1)
- NCP For CHF 3 Activity IntoleranceDocument2 pagesNCP For CHF 3 Activity IntoleranceAngelyn ArdinesNo ratings yet
- Nursing Care Plan 1 DiagDocument4 pagesNursing Care Plan 1 Diagguysornngam100% (1)
- Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationsDocument3 pagesAssessment Nursing Diagnosis Planning Interventions Rationale EvaluationsAjay SupanNo ratings yet
- NCP Cad ElectiveDocument1 pageNCP Cad ElectivejoegeNo ratings yet
- Data Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDocument4 pagesData Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDienizs LabiniNo ratings yet
- Ineffective Tissue Perfusion Related To Decrease Hemoglobin Concentration in The BloodDocument2 pagesIneffective Tissue Perfusion Related To Decrease Hemoglobin Concentration in The BloodKit Alizon BarredoNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainNathalie kate petallarNo ratings yet
- Assessment Diagnosis Scientific Explanation Objective Interventions Rationale Expected Outcome Short Term: Short TermDocument4 pagesAssessment Diagnosis Scientific Explanation Objective Interventions Rationale Expected Outcome Short Term: Short TermGensen Cu RoxasNo ratings yet
- NCP 1: Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Cerebrovascular AccidentDocument14 pagesNCP 1: Ineffective Cerebral Tissue Perfusion Related To Interruption of Blood Flow Secondary To Cerebrovascular AccidentKyle Jingco100% (2)
- B. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelDocument2 pagesB. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelCarl Elexer Cuyugan Ano50% (2)
- Hydatidiform Mole Study GuideDocument4 pagesHydatidiform Mole Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" IntroDocument6 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" IntroCarl Elexer Cuyugan AnoNo ratings yet
- CarlncmDocument2 pagesCarlncmCarl Elexer Cuyugan AnoNo ratings yet
- Ectopic Pregnancy Study GuideDocument5 pagesEctopic Pregnancy Study GuideCarl Elexer Cuyugan Ano100% (1)
- Diversity of Microorganisms 2Document71 pagesDiversity of Microorganisms 2Carl Elexer Cuyugan Ano100% (4)
- Nurse0710 PampangaDocument135 pagesNurse0710 PampangaproffsgNo ratings yet
- Neonatal Sepsis (Sepsis Neonatorum) Medical Management Not Included...Document29 pagesNeonatal Sepsis (Sepsis Neonatorum) Medical Management Not Included...Carl Elexer Cuyugan Ano100% (3)
- Traumatic Brain Injuries Study GuideDocument18 pagesTraumatic Brain Injuries Study GuideCarl Elexer Cuyugan Ano100% (1)
- Iii. Patient and His Illness A. Review of Anatomy and PhysiologyDocument13 pagesIii. Patient and His Illness A. Review of Anatomy and PhysiologyCarl Elexer Cuyugan AnoNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- Shapes and Arrangements of BacteriaDocument22 pagesShapes and Arrangements of BacteriaCarl Elexer Cuyugan Ano100% (3)
- Microbial Physiology and Genetics Part 1Document43 pagesMicrobial Physiology and Genetics Part 1Carl Elexer Cuyugan Ano100% (7)
- Hypertension Study GuideDocument4 pagesHypertension Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- Craniotomy Surgical Case ReportDocument58 pagesCraniotomy Surgical Case ReportCarl Elexer Cuyugan Ano100% (9)
- Principles of Antimicrobial Therapy Part 1Document83 pagesPrinciples of Antimicrobial Therapy Part 1Carl Elexer Cuyugan Ano100% (1)
- Diversity of Microorganisms 1 - AcellularDocument39 pagesDiversity of Microorganisms 1 - AcellularCarl Elexer Cuyugan Ano100% (1)
- Diversity of Microorganisms 1 - ProkaryoticDocument45 pagesDiversity of Microorganisms 1 - ProkaryoticCarl Elexer Cuyugan Ano100% (6)
- The Metabolic and Endocrine Systems NotesDocument9 pagesThe Metabolic and Endocrine Systems NotesCarl Elexer Cuyugan Ano100% (2)
- Cell Structure and TaxonomyDocument50 pagesCell Structure and TaxonomyCarl Elexer Cuyugan AnoNo ratings yet
- Basic Drug Computations Part 1Document8 pagesBasic Drug Computations Part 1Carl Elexer Cuyugan Ano100% (4)
- Gastrointestinal Tract System NotesDocument8 pagesGastrointestinal Tract System NotesCarl Elexer Cuyugan Ano100% (1)
- Complications of Intravenous TherapyDocument37 pagesComplications of Intravenous TherapyCarl Elexer Cuyugan Ano100% (3)
- Basic Computations 2 IV & IVFDocument37 pagesBasic Computations 2 IV & IVFCarl Elexer Cuyugan Ano100% (5)
- The Contemporary Relational Supervisor 2Nd Edition Robert Ernest Lee Thorana Strever Nelson Online Ebook Texxtbook Full Chapter PDFDocument69 pagesThe Contemporary Relational Supervisor 2Nd Edition Robert Ernest Lee Thorana Strever Nelson Online Ebook Texxtbook Full Chapter PDFwilliam.roper672100% (6)
- Ch. 2 - Questions Flashcards by Brian Weldon - BrainscapeDocument10 pagesCh. 2 - Questions Flashcards by Brian Weldon - BrainscapeKay MendozaNo ratings yet
- Mental Health & Psychiatric NursingDocument617 pagesMental Health & Psychiatric NursingEVERYTHING TvNo ratings yet
- Week 7 ExamDocument5 pagesWeek 7 ExamKevin NyasogoNo ratings yet
- Safety Leadership NewDocument35 pagesSafety Leadership NewdhabriNo ratings yet
- Catalogo BlueSAODocument132 pagesCatalogo BlueSAOJuan CeballosNo ratings yet
- 21.0 - Permit To Work Systems v3.0 English (Full Permission)Document18 pages21.0 - Permit To Work Systems v3.0 English (Full Permission)Amal JagadiNo ratings yet
- NODocument8 pagesNOAbu Abbas AiyubNo ratings yet
- Новий Microsoft Word DocumentDocument3 pagesНовий Microsoft Word Documentwood swordNo ratings yet
- Introduction To Cleft Lip and Palate: Prof. Adetokunbo Adebola Aminu Kano TH / Bayero University, Kano, NigeriaDocument9 pagesIntroduction To Cleft Lip and Palate: Prof. Adetokunbo Adebola Aminu Kano TH / Bayero University, Kano, NigeriaYuan MarcelitaNo ratings yet
- Pneumonia PPT NewDocument22 pagesPneumonia PPT NewOsuri MapitigamaNo ratings yet
- Redondo, I., Russell, C. y Bernal, J. (2018)Document9 pagesRedondo, I., Russell, C. y Bernal, J. (2018)Marcos EspindolaNo ratings yet
- Classicaland Operant Conditioning ANSWERSDocument3 pagesClassicaland Operant Conditioning ANSWERSNeurotic AlienNo ratings yet
- Instruction ManualDocument46 pagesInstruction ManualNaufrago WilliesNo ratings yet
- Ayusante CatalogueDocument12 pagesAyusante CatalogueAnkit Modi0% (1)
- Mood DisordersDocument25 pagesMood DisordersRence IremedioNo ratings yet
- Ielts Speaking 1 - Topic Food and HealthDocument1 pageIelts Speaking 1 - Topic Food and HealthDuyen TranNo ratings yet
- Articulo en Ingles de ErgonomiaDocument4 pagesArticulo en Ingles de ErgonomiaNohora Alexandra PINZON PLAZASNo ratings yet
- 01/25/2021 - Ernst & Young BC LTC COVID-19 Response ReviewDocument28 pages01/25/2021 - Ernst & Young BC LTC COVID-19 Response ReviewThe Vancouver SunNo ratings yet
- NURS 682 Care Coordination and Role of The Advanced Practice NurseDocument9 pagesNURS 682 Care Coordination and Role of The Advanced Practice NurseParya VNo ratings yet
- Deparmental ListDocument39 pagesDeparmental ListLiaquat RaniaNo ratings yet
- Tarot BookDocument64 pagesTarot BookK BhauNo ratings yet
- Contactos Bioseguridad Covid19Document10 pagesContactos Bioseguridad Covid19Aldo Ezequilla RamirezNo ratings yet
- Cl_XII_Summer_vacation_HW(Eng_Core)[1]Document6 pagesCl_XII_Summer_vacation_HW(Eng_Core)[1]kuntalsaikia82No ratings yet
- AACN BSN Essentials PaperDocument9 pagesAACN BSN Essentials PaperSikany S EmmanNo ratings yet
- CITATION Ann12 /L 17417Document3 pagesCITATION Ann12 /L 17417The seriNo ratings yet
- 5th Engineers Responsibility and SafetyDocument49 pages5th Engineers Responsibility and SafetyayanNo ratings yet
- April 9, 2021 Strathmore TimesDocument12 pagesApril 9, 2021 Strathmore TimesStrathmore TimesNo ratings yet
















































































































![Cl_XII_Summer_vacation_HW(Eng_Core)[1]](https://imgv2-1-f.scribdassets.com/img/document/738917279/149x198/034399bf94/1717437509?v=1)



