You might also like
- Agile Essentials You Always Wanted To Know: Self Learning ManagementFrom EverandAgile Essentials You Always Wanted To Know: Self Learning ManagementNo ratings yet
- Safety Quiz - Answer PDFDocument1 pageSafety Quiz - Answer PDFRedzwan KadirNo ratings yet
- 09-Safety Training Attendance SheetDocument1 page09-Safety Training Attendance SheetSainu Kalathingal0% (1)
- Accident Report FormDocument2 pagesAccident Report FormAF Dowell MirinNo ratings yet
- Incident / Injury Report Form: o o o o oDocument2 pagesIncident / Injury Report Form: o o o o ostjohn300100% (1)
- Module 1-B Emergency PreparednessDocument11 pagesModule 1-B Emergency PreparednessRobin RubinaNo ratings yet
- Visitor RegistrationDocument1 pageVisitor RegistrationTOPdeskNo ratings yet
- Energy Saving OpportunitiesDocument3 pagesEnergy Saving Opportunitiesshanu4sure15No ratings yet
- Accident Investigation, Reporting and Analysis: Safety Engineering and Management For MEDocument38 pagesAccident Investigation, Reporting and Analysis: Safety Engineering and Management For MEAndre De VillaNo ratings yet
- The "5S" Philosophy: G. Lakshmi NarayananDocument51 pagesThe "5S" Philosophy: G. Lakshmi NarayanananbarasanNo ratings yet
- PCM Checklist - Camp HygieneDocument6 pagesPCM Checklist - Camp HygieneaymenmoatazNo ratings yet
- Why Why AnalysisDocument20 pagesWhy Why AnalysisAmar ReddyNo ratings yet
- IT Skill Retention PDFDocument6 pagesIT Skill Retention PDFtalalarayaratamaraNo ratings yet
- December-22 (Week-1)Document11 pagesDecember-22 (Week-1)pabitra pandaNo ratings yet
- Weekly Safety Report: Previous Total Safe Man Hour Safe Man Hours Safe Man Hours To DateDocument1 pageWeekly Safety Report: Previous Total Safe Man Hour Safe Man Hours Safe Man Hours To DateCecillia F ObejasNo ratings yet
- General Safety Incident Reporting ProcessDocument1 pageGeneral Safety Incident Reporting ProcessFredrick OganoNo ratings yet
- Daily Work MGT Sheet & FormatsDocument5 pagesDaily Work MGT Sheet & FormatsKushagra NagrathNo ratings yet
- Safety Report Sample FormatDocument16 pagesSafety Report Sample FormatgomertweeNo ratings yet
- How To Conduct An Incident InvestigationDocument4 pagesHow To Conduct An Incident Investigationkenoly123No ratings yet
- Supervisor's Incident/Accident Analysis: Oregon Military DepartmentDocument5 pagesSupervisor's Incident/Accident Analysis: Oregon Military DepartmentAnonymous m39OcDL2XnNo ratings yet
- Mockdrill ReportDocument3 pagesMockdrill Reportjanak doshiNo ratings yet
- Factories Act 1948Document70 pagesFactories Act 1948akanungoNo ratings yet
- 5S Implementation Manual Part 2Document63 pages5S Implementation Manual Part 2jgprasadNo ratings yet
- ErgonomicsDocument67 pagesErgonomicsAli ArsalanNo ratings yet
- Sample Template - Safety-DashboardDocument6 pagesSample Template - Safety-DashboardSivakumar ENo ratings yet
- Assignment Safety Report WALTON Factory Mahmudul HaqueDocument28 pagesAssignment Safety Report WALTON Factory Mahmudul Haquepunter07No ratings yet
- Incident Checklist: Other ActionsDocument1 pageIncident Checklist: Other Actionsloveson709No ratings yet
- B-711 Purpose: Agency Name Chapter No./Name Part No./Name Section No./Name Document No./Name Dates Issue EffectiveDocument3 pagesB-711 Purpose: Agency Name Chapter No./Name Part No./Name Section No./Name Document No./Name Dates Issue EffectiveJoyjoy C LbanezNo ratings yet
- Occupational Health and Safety Management System (OSHAS 18001)Document8 pagesOccupational Health and Safety Management System (OSHAS 18001)rslapena100% (1)
- Occupational Health and Safety Assessment of The Industries in Bhutan: A Three Years' Trend AnalysisDocument7 pagesOccupational Health and Safety Assessment of The Industries in Bhutan: A Three Years' Trend AnalysisAdvanced Research PublicationsNo ratings yet
- ESH Compliance Check List: Noise ControlDocument1 pageESH Compliance Check List: Noise ControlRichard BaileyNo ratings yet
- 6S in HealthcareDocument13 pages6S in HealthcareChannel MedicalNo ratings yet
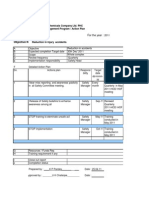
- Safety Dept. Action Plan Based On Annual Objectives 2011Document22 pagesSafety Dept. Action Plan Based On Annual Objectives 2011kirandevi1981No ratings yet
- 5 Personal Protective EquipmentDocument45 pages5 Personal Protective Equipmentdroffilcz27100% (1)
- Workshop Inspection Checklist January 2012Document12 pagesWorkshop Inspection Checklist January 2012Sundara MoorthyNo ratings yet
- Workers Seriously Injured in Conveyor AccidentsDocument2 pagesWorkers Seriously Injured in Conveyor AccidentsGissmoNo ratings yet
- Chapter 9. Failure Root Cause PreventionDocument23 pagesChapter 9. Failure Root Cause PreventionAbdirahman Ali mohamudNo ratings yet
- Integr Ted Business Re S: at SourceDocument14 pagesIntegr Ted Business Re S: at SourcecyclopsoctopusNo ratings yet
- Safety Week Kalwa 2020Document3 pagesSafety Week Kalwa 2020Amit MarothiyaNo ratings yet
- Red Tag Red Tag Red Tag: Log No. Log No. Log NoDocument1 pageRed Tag Red Tag Red Tag: Log No. Log No. Log NovishvendanNo ratings yet
- 2019-01 WRAP Pre-Audit Self-Assessment English Fillable PROTECTEDDocument84 pages2019-01 WRAP Pre-Audit Self-Assessment English Fillable PROTECTEDDark Prince DukeNo ratings yet
- Checklist (BOCW) Act 1996 V0.1.3Document2 pagesChecklist (BOCW) Act 1996 V0.1.3Imran Mulani100% (1)
- Vehicle Inspection: Administrative Procedures & GuidelinesDocument1 pageVehicle Inspection: Administrative Procedures & GuidelinesAdi Mbah Rowo WibowoNo ratings yet
- Accident PreventionDocument71 pagesAccident PreventionSubhransu MohapatraNo ratings yet
- A 2 Housekeeping ScheduleDocument2 pagesA 2 Housekeeping Schedulebrian pilapilNo ratings yet
- Premobilisation Wheel Loader InspectionDocument1 pagePremobilisation Wheel Loader InspectionArjun Satheesan100% (1)
- Milling MachineDocument1 pageMilling MachineFikri MaulanaNo ratings yet
- Compound Machine ReportDocument9 pagesCompound Machine Reportapi-300746898No ratings yet
- Form Red TagDocument1 pageForm Red TagAputMartinNo ratings yet
- String Diagram and Plant Layout: Group - 2Document25 pagesString Diagram and Plant Layout: Group - 2VaanazhaganNo ratings yet
- Ergonomics 2018 CAMLT FINAL PDFDocument93 pagesErgonomics 2018 CAMLT FINAL PDFchaerul.anwar554No ratings yet
- Safety Training Presentations: Good HousekeepingDocument23 pagesSafety Training Presentations: Good HousekeepingAhmet SenlerNo ratings yet
- Equipment Operating ProcedureDocument5 pagesEquipment Operating ProcedurezaizamNo ratings yet
- Safety WeekDocument3 pagesSafety Weekmukeshkatarnavare0% (1)
- Accident-Incident Investigation ProcedureDocument2 pagesAccident-Incident Investigation Procedureishaharom100% (1)
- Safety Park BungeDocument37 pagesSafety Park BungeRavi Sankar VenkatesanNo ratings yet
- Pantry Checklist: Name: Date: S. No. Checklist Statu SDocument1 pagePantry Checklist: Name: Date: S. No. Checklist Statu SKhanna MulberryNo ratings yet
- F-OPN-07-17 Property Gate Pass (Rev. 00)Document2 pagesF-OPN-07-17 Property Gate Pass (Rev. 00)diane laine loretoNo ratings yet
- Incident Report FormDocument1 pageIncident Report FormVeronica AlbairaNo ratings yet
- Accident Report FormDocument4 pagesAccident Report FormAJAY1381No ratings yet