You might also like
- Urology MCQsDocument13 pagesUrology MCQsRahmah Shah Bahai83% (6)
- Nokia 7750 SR-a Service Router Customer Overview Presentation (Level 1)Document38 pagesNokia 7750 SR-a Service Router Customer Overview Presentation (Level 1)NisaiyhoutNo ratings yet
- Lung CancerDocument19 pagesLung Cancerj.doe.hex_87No ratings yet
- Powerpoint: Liver Surgical DiseasesDocument95 pagesPowerpoint: Liver Surgical Diseasesj.doe.hex_8792% (12)
- Green Book, Methods For The Determination of Possible Damage, CPR 16EDocument337 pagesGreen Book, Methods For The Determination of Possible Damage, CPR 16Ejeremyg998100% (8)
- James Lewis - Witchcraft Today An Encyclopedia of Wiccan and Neopagan TraditionsDocument424 pagesJames Lewis - Witchcraft Today An Encyclopedia of Wiccan and Neopagan Traditionsdivinskry100% (2)
- Radiology of The Urinary SystemDocument78 pagesRadiology of The Urinary Systemapi-19916399No ratings yet
- Dysplasia & Multicystic KidneyDocument8 pagesDysplasia & Multicystic KidneyShintia MalindaNo ratings yet
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDocument67 pagesObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNo ratings yet
- Kidney DisordersDocument14 pagesKidney Disordershussain AltaherNo ratings yet
- UrolithasisDocument58 pagesUrolithasisHELL RISER GAMINGNo ratings yet
- Urology1 UPDATEDDocument44 pagesUrology1 UPDATEDmarwanNo ratings yet
- Ivp Intravenous PyelographyDocument16 pagesIvp Intravenous PyelographyLuisa ManaloNo ratings yet
- NMT11 Urology Special NoteDocument36 pagesNMT11 Urology Special NoteYiba Zul100% (4)
- CT Abdomen - Hosiana O W - 42180258Document18 pagesCT Abdomen - Hosiana O W - 42180258HOSIANAOWNo ratings yet
- Mnlkaxi QH: Manisha M.Sc. NursingDocument57 pagesMnlkaxi QH: Manisha M.Sc. NursingManisha ShakyaNo ratings yet
- StoneDocument7 pagesStoneAbdul HaiNo ratings yet
- Scanning Technique of KidneysDocument103 pagesScanning Technique of KidneysPhuntsho OngmoNo ratings yet
- The Liver: Methods of ExaminationDocument49 pagesThe Liver: Methods of Examinationj.doe.hex_87No ratings yet
- Urology Notes 1Document43 pagesUrology Notes 1Shazaan NadeemNo ratings yet
- Hydronephrosis OutlineDocument13 pagesHydronephrosis OutlineSarah Sy-SantosNo ratings yet
- Investigation JF The Urinary TractDocument139 pagesInvestigation JF The Urinary TractВладимир КурпаянидиNo ratings yet
- ABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Document26 pagesABDOMINAL AND PELVIC MASSES IN PEDIATRICS - Level 4Malueth AnguiNo ratings yet
- Carcinoma Pancreas and Periampullary RegionDocument37 pagesCarcinoma Pancreas and Periampullary RegionlallsNo ratings yet
- Info DcsDocument9 pagesInfo DcsKhei Laqui SNNo ratings yet
- HydronephrosisDocument43 pagesHydronephrosisjessyNo ratings yet
- Pathophysiology of Ureteral CalculiDocument14 pagesPathophysiology of Ureteral CalculiEdmel Pamplona DuquesaNo ratings yet
- 5 - Malformations of The Urinary System With Violation of UrodynamicsDocument4 pages5 - Malformations of The Urinary System With Violation of UrodynamicsKatalinNo ratings yet
- Ureterocele 130919225917 Phpapp02Document23 pagesUreterocele 130919225917 Phpapp02Marcelo Bravo CortesNo ratings yet
- Anomalies of The Upper Urinary TractDocument6 pagesAnomalies of The Upper Urinary TractMohamed Al-zichrawyNo ratings yet
- Congenital Anomalies of Kidney and Urinary TractDocument53 pagesCongenital Anomalies of Kidney and Urinary TractDoctor peds100% (1)
- UrolithiasisDocument29 pagesUrolithiasis143bb100% (1)
- Questions in Urologic Radiology For Medical StudentsDocument89 pagesQuestions in Urologic Radiology For Medical StudentsNicolae TsybyrnaNo ratings yet
- IVPDocument48 pagesIVPDini Lintangsari100% (1)
- 10 KidneysDocument6 pages10 KidneysMark PadulloNo ratings yet
- HydronephrosisDocument7 pagesHydronephrosisNaqash NobleNo ratings yet
- Radiological Investigation of The Biliary Tract: 1-Plain RadiographDocument11 pagesRadiological Investigation of The Biliary Tract: 1-Plain Radiographhussain AltaherNo ratings yet
- Anomalies of Rotation To CDDocument15 pagesAnomalies of Rotation To CDGren May Angeli MagsakayNo ratings yet
- Master Radiology Notes UrologyDocument106 pagesMaster Radiology Notes UrologySafwan ShaikhNo ratings yet
- Imaging in Paediatric UTIDocument30 pagesImaging in Paediatric UTIChua Kai XiangNo ratings yet
- Liver Disease: Schwartz Principles of Surgery2010Document50 pagesLiver Disease: Schwartz Principles of Surgery2010ralphNo ratings yet
- Ms 2 PointersDocument4 pagesMs 2 PointersJINYVEV APARICINo ratings yet
- Wilm's Tumor RadiographyDocument8 pagesWilm's Tumor RadiographyWowo Masthuro MahfudNo ratings yet
- 1-Urinary Tract Imaging TechniquesDocument27 pages1-Urinary Tract Imaging TechniquesallordNo ratings yet
- PRACTICAL EXAM PPT RadiologyDocument51 pagesPRACTICAL EXAM PPT RadiologyPartha Ganesan0% (1)
- 54.the Gallbladder and Bile DuctsDocument19 pages54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondNo ratings yet
- Renal Pathology Blok 13Document71 pagesRenal Pathology Blok 13Arsy Mira PertiwiNo ratings yet
- IVU - DR Juned A AnsariDocument50 pagesIVU - DR Juned A AnsariJuned A AnsariNo ratings yet
- Renal CellDocument1 pageRenal Cellmohammedhosney99999No ratings yet
- Urogenital RadiologyDocument3 pagesUrogenital RadiologyAbedinego MalukaNo ratings yet
- Symptomatology of GUT DisordersDocument75 pagesSymptomatology of GUT DisordersMaraJoRNNo ratings yet
- Renal Session 2 PDFDocument101 pagesRenal Session 2 PDFDokki ScanNo ratings yet
- Autopsy 2Document106 pagesAutopsy 2gimspath cme2022No ratings yet
- Nephrolithiasis PDFDocument16 pagesNephrolithiasis PDFApriany Cordias Arlita SilalahiNo ratings yet
- SURG - Hepatobiliary, Pancreas, SpleenDocument230 pagesSURG - Hepatobiliary, Pancreas, SpleenJoan Timbol100% (1)
- 20 - Pediatric Urinary DisordersDocument62 pages20 - Pediatric Urinary DisordersKhaalid AbdirahmanNo ratings yet
- Tractus UrinariusDocument23 pagesTractus UrinariusYaleswari Hayu PertiwiNo ratings yet
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Kub IvpDocument46 pagesKub IvpBryJos tiongsonNo ratings yet
- Uro RadiologyDocument78 pagesUro RadiologyDavid Ogechi Atandi100% (1)
- Renal Cancers - Shalom - 2Document30 pagesRenal Cancers - Shalom - 2Bryan FjbNo ratings yet
- CAKUTDocument50 pagesCAKUTsantosh subediNo ratings yet
- Categories of Malformations: Anomalies of Number, Volume and Structure Ascent, Form and Fusion, Rotation andDocument3 pagesCategories of Malformations: Anomalies of Number, Volume and Structure Ascent, Form and Fusion, Rotation andÁngel Parra CominoNo ratings yet
- Clinical Examination of Genitourinary SystemDocument43 pagesClinical Examination of Genitourinary SystemKeamina .aNo ratings yet
- Namaz - The Health BenefitsDocument130 pagesNamaz - The Health Benefitsj.doe.hex_87100% (1)
- Nutrition in InfantDocument7 pagesNutrition in Infantj.doe.hex_87No ratings yet
- Lecture2c MdsyndromesDocument2 pagesLecture2c Mdsyndromesj.doe.hex_87No ratings yet
- Atherosclerosis. Biochemical Modifications in Acute Coronary SyndromeDocument12 pagesAtherosclerosis. Biochemical Modifications in Acute Coronary Syndromej.doe.hex_87No ratings yet
- Svaritm 2010Document26 pagesSvaritm 2010j.doe.hex_87No ratings yet
- Aplast AnDocument9 pagesAplast Anj.doe.hex_87No ratings yet
- Understanding The 12 - Lead ECG, Part IIDocument11 pagesUnderstanding The 12 - Lead ECG, Part IIj.doe.hex_87No ratings yet
- Hydatid Disease: or Iceberg SignDocument53 pagesHydatid Disease: or Iceberg Signj.doe.hex_87No ratings yet
- Understanding The 12 - Lead ECG, Part 1Document9 pagesUnderstanding The 12 - Lead ECG, Part 1j.doe.hex_87No ratings yet
- Aplastic Anemia, 2008Document10 pagesAplastic Anemia, 2008j.doe.hex_87No ratings yet
- Studies Suggest That Myocarditis Is A: Important Causes of MyocarditisDocument11 pagesStudies Suggest That Myocarditis Is A: Important Causes of MyocarditisCristina Georgiana CoticăNo ratings yet
- The Liver: Methods of ExaminationDocument49 pagesThe Liver: Methods of Examinationj.doe.hex_87No ratings yet
- Powerpoint: Gall Stone Disease and Related DisordersDocument70 pagesPowerpoint: Gall Stone Disease and Related Disordersj.doe.hex_8767% (3)
- Radiology - Imaging of The ThoraxDocument49 pagesRadiology - Imaging of The Thoraxj.doe.hex_87No ratings yet
- Cardiac Imaging TechniquesDocument86 pagesCardiac Imaging Techniquesj.doe.hex_87No ratings yet
- Radiology - Imaging of The ThoraxDocument49 pagesRadiology - Imaging of The Thoraxj.doe.hex_87No ratings yet
- Water and Electrolytes DisturbancesDocument63 pagesWater and Electrolytes Disturbancesj.doe.hex_87No ratings yet
- Lionte Cor Pulmonale2010Document11 pagesLionte Cor Pulmonale2010j.doe.hex_87No ratings yet
- Lecture 1 Chest TraumaDocument19 pagesLecture 1 Chest Traumaj.doe.hex_870% (1)
- Powerpoint: Chronic Inflammatory DisordesDocument55 pagesPowerpoint: Chronic Inflammatory Disordesj.doe.hex_87No ratings yet
- Endocrinology Pharmacology: Hormone Agonists, Antagonists & ModulatorsDocument151 pagesEndocrinology Pharmacology: Hormone Agonists, Antagonists & Modulatorsj.doe.hex_87100% (1)
- Photosynthesis Lab Report ExampleDocument2 pagesPhotosynthesis Lab Report ExampleTiffany RishiNo ratings yet
- Astm e 1044 - 96Document2 pagesAstm e 1044 - 96MarceloNo ratings yet
- Scope of Works by ChainageDocument1 pageScope of Works by ChainageMohd Kamal TajudinNo ratings yet
- DIM Document Primescan Clinical Studies Overview ENDocument22 pagesDIM Document Primescan Clinical Studies Overview ENrita adhikariNo ratings yet
- 10 MW Thermal EnergyDocument3 pages10 MW Thermal EnergyDeepal DhamejaNo ratings yet
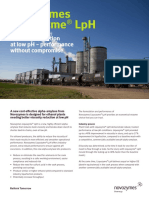
- Liquozyme LPH Benefit SheetDocument2 pagesLiquozyme LPH Benefit SheetcamilodomesaNo ratings yet
- Project GraphicsDocument10 pagesProject GraphicsProject GraphicsNo ratings yet
- Design Calculation or Analysis Cover Sheet SSC: Iz!-E-GfDocument20 pagesDesign Calculation or Analysis Cover Sheet SSC: Iz!-E-GfPawan TiwariNo ratings yet
- Wolaita Sodo University: Student Name: IdDocument62 pagesWolaita Sodo University: Student Name: IdMulugetaNo ratings yet
- Range Rover Evoque BrochureDocument2 pagesRange Rover Evoque BrochureParantap SinghNo ratings yet
- Week 3 Case - DOBDocument3 pagesWeek 3 Case - DOBKirk Matthew ZhuNo ratings yet
- The Najd Fault System, Arabian ShieldDocument28 pagesThe Najd Fault System, Arabian Shieldgeo ghallabNo ratings yet
- Puran c1Document22 pagesPuran c1dennis gamisNo ratings yet
- Drug Study: Francisco Tampos JRDocument37 pagesDrug Study: Francisco Tampos JRCarlmeister Ambray JudillaNo ratings yet
- CaractTécnicas3 FreeStyleDocument2 pagesCaractTécnicas3 FreeStyleMauricioSantoyoNo ratings yet
- Pricomm FinalsDocument8 pagesPricomm FinalsAllyza Marie BalaneNo ratings yet
- WELCOME!!!!!: Six-Day Skills Enhancement Training For The TLE, TVL, ALS & Mobile TeachersDocument65 pagesWELCOME!!!!!: Six-Day Skills Enhancement Training For The TLE, TVL, ALS & Mobile TeachersErma JalemNo ratings yet
- LTJournal V20N4 02 DF LT3652 Jay - CelaniDocument6 pagesLTJournal V20N4 02 DF LT3652 Jay - CelaniCanerNo ratings yet
- Sony MHC rg551s Manual de Usuario PDFDocument48 pagesSony MHC rg551s Manual de Usuario PDFNelson ContrerasNo ratings yet
- Indonesia'S Capital Market Updates: Akhmad NuranyantoDocument35 pagesIndonesia'S Capital Market Updates: Akhmad NuranyantoSiti Hutami pratiwiNo ratings yet
- 6th Sem Mech Mid Sem Question Bank-1Document14 pages6th Sem Mech Mid Sem Question Bank-1dharmeshNo ratings yet
- ISCP Aerospace Handbook 19 21Document33 pagesISCP Aerospace Handbook 19 21Dibya DillipNo ratings yet
- Swami SivanandaDocument276 pagesSwami SivanandaJames Herring100% (1)
- RAN17.1 Basic Feature DescriptionDocument234 pagesRAN17.1 Basic Feature Descriptiondonia77No ratings yet
- Topic 16 Types of Electric Circuit ComponentsDocument6 pagesTopic 16 Types of Electric Circuit ComponentsSunNo ratings yet
- Analysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationDocument4 pagesAnalysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationMahavir GemavatNo ratings yet
- IBM TapeDocument11 pagesIBM TapeDaWheng VargasNo ratings yet