You might also like
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- OSCE - Health PromotionDocument13 pagesOSCE - Health PromotionbabukanchaNo ratings yet
- Rests Rest SeatsDocument42 pagesRests Rest SeatsSahana RangarajanNo ratings yet
- Occlusion in Complete DentureDocument64 pagesOcclusion in Complete Denturepuja singhNo ratings yet
- Relining and RebasingDocument5 pagesRelining and RebasingMarwaAmerNo ratings yet
- Classification and Impression Techniques of ImplantsDocument72 pagesClassification and Impression Techniques of ImplantsvanillalavenderNo ratings yet
- Fundamentals of Fixed Prosthodontics P 4355700Document3 pagesFundamentals of Fixed Prosthodontics P 4355700Lorin Columb100% (1)
- Impression C DDocument48 pagesImpression C DZaid KhameesNo ratings yet
- Impression Tech in FPDDocument50 pagesImpression Tech in FPDDrGagandeep SinghNo ratings yet
- Managing Problems in Complete Dentures - LectureDocument18 pagesManaging Problems in Complete Dentures - LectureMarlisa Zhong100% (1)
- Partial Retainer in FPD DR VikasDocument99 pagesPartial Retainer in FPD DR VikasVikas AggarwalNo ratings yet
- Relining and Rebasing of Complete Dentures: Bds MSC MRD Rcsed 4 Year/removable Prosthodontics 441-442Document33 pagesRelining and Rebasing of Complete Dentures: Bds MSC MRD Rcsed 4 Year/removable Prosthodontics 441-442Aya ShahrouriNo ratings yet
- Relining & RebasingDocument86 pagesRelining & RebasingJASPREETKAUR0410100% (1)
- Cast PostDocument3 pagesCast PostsmilekkmNo ratings yet
- Presentation1 130907161730Document222 pagesPresentation1 130907161730Radu RîcăNo ratings yet
- Luting Agents For Fixed Prosthodontics / Orthodontic Courses by Indian Dental AcademyDocument37 pagesLuting Agents For Fixed Prosthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Orientation Jaw Relation ProsthoDocument24 pagesOrientation Jaw Relation ProsthoFourthMolar.comNo ratings yet
- Relining and Rebasing in Complete Dentures: Indian Dental AcademyDocument59 pagesRelining and Rebasing in Complete Dentures: Indian Dental AcademyNajeeb UllahNo ratings yet
- Special Tray Fabrication-130912012832-Phpapp01Document26 pagesSpecial Tray Fabrication-130912012832-Phpapp01OTNo ratings yet
- Hobo Technique PDFDocument8 pagesHobo Technique PDFAmar BimavarapuNo ratings yet
- Final Biomechanics of Edentulous StateDocument114 pagesFinal Biomechanics of Edentulous StateSnigdha SahaNo ratings yet
- Different Pontic DesignDocument5 pagesDifferent Pontic DesignHassanein Al-HamdaniNo ratings yet
- Applied Anatomy Related To Complete Denture-Maxilla MandibleDocument57 pagesApplied Anatomy Related To Complete Denture-Maxilla MandibleRen Jye ChongNo ratings yet
- Anatomy and Physiology in Relation To Complete Denture ConstructionDocument4 pagesAnatomy and Physiology in Relation To Complete Denture ConstructionCyril Almario CunananNo ratings yet
- 24-Sequelae of Wearing Complete Dentures - Rajat DangDocument19 pages24-Sequelae of Wearing Complete Dentures - Rajat DangNaunit Vaid100% (1)
- Unconventional Complete Dentures: Innovative Approach in ProsthodonticsDocument10 pagesUnconventional Complete Dentures: Innovative Approach in ProsthodonticsAastha DuaNo ratings yet
- Identification of Complete Denture Problems: A Summary: ProstheticsDocument7 pagesIdentification of Complete Denture Problems: A Summary: ProstheticsPolo RalfNo ratings yet
- Factors Which Complicate Impression Making PDFDocument18 pagesFactors Which Complicate Impression Making PDFMostafa FayadNo ratings yet
- Clinical Management of Aquired Defects of MaxillaDocument81 pagesClinical Management of Aquired Defects of Maxillarayavarapu sunilNo ratings yet
- The Retention of Complete DentureDocument15 pagesThe Retention of Complete DentureAmit ShivrayanNo ratings yet
- Finishing and Polishing Materials.9Document8 pagesFinishing and Polishing Materials.9Eman Azmi OmarNo ratings yet
- Cantor and Curtis ClassificationDocument4 pagesCantor and Curtis ClassificationMuhammad AwaisNo ratings yet
- Terminology of OcclusionDocument6 pagesTerminology of OcclusionShyam K MaharjanNo ratings yet
- Contacts and ContoursDocument73 pagesContacts and ContoursKasturi VenkateswarluNo ratings yet
- Basic Principles in Impression Making M M DevanDocument6 pagesBasic Principles in Impression Making M M Devanmfaheemuddin85100% (1)
- A Hollow Bulb ObturatorDocument6 pagesA Hollow Bulb ObturatorrekabiNo ratings yet
- Fabrication of Record BaseDocument38 pagesFabrication of Record BaseSuvasish SuvasishNo ratings yet
- Denture Lining MaterialsDocument47 pagesDenture Lining MaterialsTooba NadeemNo ratings yet
- Teeth Selection and ArrangementDocument118 pagesTeeth Selection and Arrangementaakankshakanwar100% (2)
- Cheeck PlumperDocument44 pagesCheeck PlumperAnuRaveendranNo ratings yet
- Impression Techniques in RPDDocument82 pagesImpression Techniques in RPDpramodaniNo ratings yet
- Impression Procedures in CD - KIRTI SHARMADocument42 pagesImpression Procedures in CD - KIRTI SHARMAKirti SharmaNo ratings yet
- Selecion of Major ConnectorsDocument2 pagesSelecion of Major ConnectorsTanmay SrivastavaNo ratings yet
- Swing Lock Partial DentureDocument22 pagesSwing Lock Partial DentureSanNo ratings yet
- Examination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsDocument73 pagesExamination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsMohamedNo ratings yet
- Repair of Complete DenturesDocument25 pagesRepair of Complete Denturesjohn mwambu67% (3)
- Intracoronal Restorations in FPDDocument60 pagesIntracoronal Restorations in FPDChandni SetiaNo ratings yet
- Intro To RPDDocument68 pagesIntro To RPDJamesJakeNo ratings yet
- Perio Restorative Inter Relationship (Perio)Document44 pagesPerio Restorative Inter Relationship (Perio)FourthMolar.com75% (4)
- Implant Systems: Dr. Unjum Bashir, Dr. Manas Gupta, Dr. Ravish AhujaDocument7 pagesImplant Systems: Dr. Unjum Bashir, Dr. Manas Gupta, Dr. Ravish AhujaDr FarhatNo ratings yet
- Articulators Through The Years Revisited From 1971Document9 pagesArticulators Through The Years Revisited From 1971Nicco MarantsonNo ratings yet
- Direct RetainersDocument10 pagesDirect RetainersSakinah SyahirahNo ratings yet
- Failures in FPDDocument30 pagesFailures in FPDMayank Aggarwal100% (1)
- Post Insertion Problem and Its ManagmentDocument108 pagesPost Insertion Problem and Its Managmentranjeet kumar chaudharyNo ratings yet
- Principles of Tooth PreparationDocument10 pagesPrinciples of Tooth Preparationruchika100% (2)
- Post Insertion Complaints in CD For Dental Students For Final Year For Their Seminar.Document31 pagesPost Insertion Complaints in CD For Dental Students For Final Year For Their Seminar.Anonymous ceYk4p4No ratings yet
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- My Dentist and the Tooth Fairy: Activity and Coloring BookFrom EverandMy Dentist and the Tooth Fairy: Activity and Coloring BookNo ratings yet
- Providers 202310200719Document26 pagesProviders 202310200719Vamsi Krishna GarimellaNo ratings yet
- Tetric LineDocument10 pagesTetric LineAndrea LawNo ratings yet
- Long-Term Pro File Attractiveness in Class II Division 1 Malocclusion Patients Treated With and Without ExtractionsDocument10 pagesLong-Term Pro File Attractiveness in Class II Division 1 Malocclusion Patients Treated With and Without ExtractionsMarlon Cespedes AlccaNo ratings yet
- Bicon Seating ChecklistDocument2 pagesBicon Seating ChecklistAnna BuzdugaNo ratings yet
- Internalfit: Simplicity Made AccessibleDocument2 pagesInternalfit: Simplicity Made AccessibleCris GshsuwNo ratings yet
- Shirley PDFDocument8 pagesShirley PDFANDREA R.GSNo ratings yet
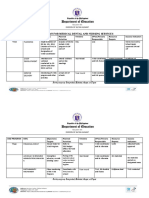
- Sample WINS Action PLanDocument3 pagesSample WINS Action PLanJEANYVIE ESPINOSANo ratings yet
- Nanda Archwires: Science Does Matter!Document2 pagesNanda Archwires: Science Does Matter!aung NaingmyoNo ratings yet
- HIV Case StudyDocument6 pagesHIV Case StudyCruz, Donna Angela M.No ratings yet
- Implantloading 1 161213182754 PDFDocument147 pagesImplantloading 1 161213182754 PDFSudhanshu Kumar KashyapNo ratings yet
- Cephalometric File: Batch: 2009-2012Document6 pagesCephalometric File: Batch: 2009-2012MariyamNo ratings yet
- Treatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceDocument9 pagesTreatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceJuan Carlos MeloNo ratings yet
- Dental Burs in Restorative Dentistry and Endodonticspast and Present A ReviewDocument8 pagesDental Burs in Restorative Dentistry and Endodonticspast and Present A ReviewAshyana SaeedNo ratings yet
- Capstone Project FinalDocument16 pagesCapstone Project Finalapi-409052955No ratings yet
- Normal Periodontium 1Document49 pagesNormal Periodontium 1mdio midoNo ratings yet
- DentalDocument7 pagesDentalPaul SmithNo ratings yet
- Occlusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumDocument4 pagesOcclusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumTung Thanh NguyenNo ratings yet
- Dental Laboratory Procedures CompleteDocument597 pagesDental Laboratory Procedures CompleteDINESH VENKATESANNo ratings yet
- Minimal Invasive Dentistry: Review ArticleDocument4 pagesMinimal Invasive Dentistry: Review ArticleKarissa NavitaNo ratings yet
- HEP Builder - HEP Builder PDFDocument2 pagesHEP Builder - HEP Builder PDFHazely TagasaNo ratings yet
- 2017 CHAI Incisal Preparation Design For Ceramic VeneersDocument13 pages2017 CHAI Incisal Preparation Design For Ceramic VeneersDiego Alejandro Cortés LinaresNo ratings yet
- Tooth Mousse-IADR-Ranjitkar 9-07Document1 pageTooth Mousse-IADR-Ranjitkar 9-07gabyNo ratings yet
- Communication With Dental LaboratoryDocument16 pagesCommunication With Dental Laboratorykhaled alahmadNo ratings yet
- Mini Implants For Definitive Asystmatic ReviewDocument9 pagesMini Implants For Definitive Asystmatic ReviewAeman ElkezzaNo ratings yet
- Oral Care in India: Euromonitor International April 2021Document11 pagesOral Care in India: Euromonitor International April 2021Sanjay ShambhuNo ratings yet
- Kebiasaan Merokok Dan Terjadinya Smoker's Melanosis: Iin Revien, Aurelia S. R. Supit, Pritartha S. AninditaDocument10 pagesKebiasaan Merokok Dan Terjadinya Smoker's Melanosis: Iin Revien, Aurelia S. R. Supit, Pritartha S. AninditaHasbi AshidiqyNo ratings yet
- INSISIVDocument7 pagesINSISIVLansky TrimeilanaNo ratings yet
- Double Seal PDFDocument3 pagesDouble Seal PDFJitender Reddy100% (1)