You might also like
- Postural AssessmentDocument63 pagesPostural Assessmentdariand100% (1)
- Postural AssessmentDocument64 pagesPostural AssessmentNikks BoradeNo ratings yet
- Anatomy for Strength and Fitness Training for Women: An Illustrated Guide to Your Muscles in ActionFrom EverandAnatomy for Strength and Fitness Training for Women: An Illustrated Guide to Your Muscles in ActionNo ratings yet
- PPPDocument29 pagesPPPLeon SamadiNo ratings yet
- PostureDocument85 pagesPostureDr.Debanjan Mondal (pt)100% (1)
- Body Alignment and Balance/Coordinat IonDocument39 pagesBody Alignment and Balance/Coordinat Ionim. EliasNo ratings yet
- Sajida Bibi NoonariDocument39 pagesSajida Bibi NoonariSajida Bibi NoonariNo ratings yet
- StartingPositions Derived PositionsDocument53 pagesStartingPositions Derived PositionsTobit Andre CaballoNo ratings yet
- Posture EvaluationDocument12 pagesPosture EvaluationpaconscribdNo ratings yet
- OMM Year 1Document22 pagesOMM Year 1bgav00No ratings yet
- 326 Musculoskeletal Assessment Fa10Document36 pages326 Musculoskeletal Assessment Fa10arjetahoward100% (1)
- Musician, Heal Thyself!: Free Your Shoulder Region through Body MappingFrom EverandMusician, Heal Thyself!: Free Your Shoulder Region through Body MappingNo ratings yet
- Archery Anatomy: An Introduction to Techniques for Improved PerformanceFrom EverandArchery Anatomy: An Introduction to Techniques for Improved PerformanceRating: 4 out of 5 stars4/5 (1)
- Mastering Posture A Comprehensive Guide to Optimal Body AlignmentFrom EverandMastering Posture A Comprehensive Guide to Optimal Body AlignmentNo ratings yet
- WS&C Lec2Document20 pagesWS&C Lec2Benjamin LeeNo ratings yet
- Lumbo-Pelvic Stability and Back Pain: What's The Link?Document8 pagesLumbo-Pelvic Stability and Back Pain: What's The Link?atul-heroNo ratings yet
- Body Mechanics, Alignment, and MobilityDocument42 pagesBody Mechanics, Alignment, and MobilityAbigail Filio Monge86% (7)
- Shoulder Girdle/ Gelang BahuDocument36 pagesShoulder Girdle/ Gelang BahuRizki PerdanaNo ratings yet
- 10 Minutes Abs Workout and Core Exercises for Seniors: Fully Illustrated Guide to Boost Bone Health and Lower the Risk of Falls and Injury (+200 Exercises): For Seniors, #2From Everand10 Minutes Abs Workout and Core Exercises for Seniors: Fully Illustrated Guide to Boost Bone Health and Lower the Risk of Falls and Injury (+200 Exercises): For Seniors, #2No ratings yet
- Presentation%20Document30 pagesPresentation%20Rida FatimaNo ratings yet
- Musculoskeletal AssessmentDocument69 pagesMusculoskeletal AssessmentWorku Kifle100% (2)
- Annexure 2Document58 pagesAnnexure 2Prasanth KumarNo ratings yet
- Core Stability UpdateDocument38 pagesCore Stability Updateruth sosa0% (1)
- Bad Posture - A Reason For Change in SpinalDocument58 pagesBad Posture - A Reason For Change in SpinalPooja jainNo ratings yet
- Selecting Appropriate and Effective EquipmentDocument63 pagesSelecting Appropriate and Effective EquipmentTransverse Myelitis AssociationNo ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- Applied Anatomy Unit IDocument37 pagesApplied Anatomy Unit Iapi-19916399No ratings yet
- Core MUSCLES2Document38 pagesCore MUSCLES2romancivi0% (1)
- Aarti - Introduction of Biomechanics PostureDocument64 pagesAarti - Introduction of Biomechanics PostureKalyani Savant0% (1)
- Fitness Assessment Test: Get Ready With The Following FormsDocument32 pagesFitness Assessment Test: Get Ready With The Following FormsMaricrisNo ratings yet
- Fiziologia Mainii F BunaDocument4 pagesFiziologia Mainii F BunaliluharaNo ratings yet
- Posture PDFDocument47 pagesPosture PDFslim & Fit health sudio for womenNo ratings yet
- Pelvic Tilt & Lower Crossed SyndromeDocument18 pagesPelvic Tilt & Lower Crossed SyndromeSimo AsterNo ratings yet
- CervicothoracicSpine AssessmentDocument16 pagesCervicothoracicSpine AssessmentKanika SinhaNo ratings yet
- Postural AssessmentDocument6 pagesPostural AssessmentDance For Fitness With PoojaNo ratings yet
- Anatomy and Injuries To The SpineDocument93 pagesAnatomy and Injuries To The Spineamoon12No ratings yet
- To Chronic Musculoskeletal InjuriesDocument2 pagesTo Chronic Musculoskeletal InjuriesMary Jane DumalaganNo ratings yet
- Core Strength for 50+: A Customized Program for Safely Toning Ab, Back & Oblique MusclesFrom EverandCore Strength for 50+: A Customized Program for Safely Toning Ab, Back & Oblique MusclesNo ratings yet
- 2 The Skeletal SystemDocument38 pages2 The Skeletal SystemElena IambreshichNo ratings yet
- Lecture 2 PE 101Document14 pagesLecture 2 PE 101AyanoNo ratings yet
- Apps To Functional Anatomy Lecture 6Document9 pagesApps To Functional Anatomy Lecture 6jenNo ratings yet
- Lower Crossed SyndromeDocument8 pagesLower Crossed SyndromeThaseen75% (4)
- Assessment of Posture: Prepared By: Floriza P. de Leon, PTRPDocument17 pagesAssessment of Posture: Prepared By: Floriza P. de Leon, PTRPFloriza de Leon100% (1)
- Physical Education 01: (Self Testing Activity and Gymnastics) 1 Semester SY: 2020-2021Document5 pagesPhysical Education 01: (Self Testing Activity and Gymnastics) 1 Semester SY: 2020-2021Ma. Jhysavil ArcenaNo ratings yet
- Healthy Shoulder Handbook: 100 Exercises for Treating and Preventing Frozen Shoulder, Rotator Cuff and other Common InjuriesFrom EverandHealthy Shoulder Handbook: 100 Exercises for Treating and Preventing Frozen Shoulder, Rotator Cuff and other Common InjuriesRating: 2 out of 5 stars2/5 (1)
- How To Improve Your Posture: The Importance of Posture and How To Really Change ItFrom EverandHow To Improve Your Posture: The Importance of Posture and How To Really Change ItRating: 5 out of 5 stars5/5 (2)
- Fundamental Aspects of Sitting and StandingDocument2 pagesFundamental Aspects of Sitting and StandingMeenakshi SinghNo ratings yet
- Fix FaultsDocument31 pagesFix FaultsSamehAlyNo ratings yet
- Therapeutic Exercise: The HipDocument39 pagesTherapeutic Exercise: The HipMuhammad UsmanNo ratings yet
- Hip ExaminationDocument84 pagesHip ExaminationDeepak KumarNo ratings yet
- Manual Muscle TestingDocument13 pagesManual Muscle TestingPásztai ZoltánNo ratings yet
- Lumbar HyperlordosisDocument13 pagesLumbar HyperlordosisAdriana Lucia Martinez CastillaNo ratings yet
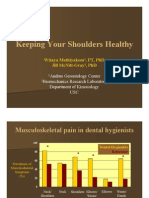
- Keeping Your Shoulders HealthyDocument38 pagesKeeping Your Shoulders Healthyxyz84No ratings yet
- MUZICADocument2 pagesMUZICAonix2000No ratings yet
- Central Line of Gravity: - Posterior 1/3 of The SkullDocument9 pagesCentral Line of Gravity: - Posterior 1/3 of The Skullonix2000No ratings yet
- Upper Limb Abductors TestDocument2 pagesUpper Limb Abductors Testonix2000No ratings yet
- Prints CRDocument1 pagePrints CRonix2000No ratings yet
- Biomecanica StretchinguluiDocument10 pagesBiomecanica Stretchinguluionix2000No ratings yet
- Anterior Posterior Line of GravityDocument5 pagesAnterior Posterior Line of Gravityonix2000No ratings yet
- AP25Document7 pagesAP25onix2000No ratings yet
- AP36Document2 pagesAP36onix2000No ratings yet
- Baroceptors Test Using The Downing TestDocument2 pagesBaroceptors Test Using The Downing Testonix2000No ratings yet
- AP41 MDocument3 pagesAP41 Monix2000No ratings yet
- Upper Limb Rotator Muscles Test: 1-Mouth Closed, Clenched Teeth, Upper Limbs Abducted 90°, HandsDocument2 pagesUpper Limb Rotator Muscles Test: 1-Mouth Closed, Clenched Teeth, Upper Limbs Abducted 90°, Handsonix2000No ratings yet
- Cross Test of The Arm Abductor Muscle & Wrist Extensor Muscles Without RotationDocument2 pagesCross Test of The Arm Abductor Muscle & Wrist Extensor Muscles Without Rotationonix2000No ratings yet
- Upper Limb Rotator Muscles Test: 1-Mouth Closed, Clenched Teeth, Upper Limbs Abducted 90°, HandsDocument2 pagesUpper Limb Rotator Muscles Test: 1-Mouth Closed, Clenched Teeth, Upper Limbs Abducted 90°, Handsonix2000No ratings yet
- Wrist Extensor Muscles TestDocument2 pagesWrist Extensor Muscles Testonix2000No ratings yet
- AP29Document3 pagesAP29onix2000No ratings yet
- AP25Document7 pagesAP25onix2000No ratings yet
- Cervical Sensor: Flexion Muscles: Infra + Supra Hyoid and Prevertebral MusclesDocument4 pagesCervical Sensor: Flexion Muscles: Infra + Supra Hyoid and Prevertebral Musclesonix2000No ratings yet
- AP26Document11 pagesAP26onix2000No ratings yet
- AP29Document3 pagesAP29onix2000No ratings yet
- Cutaneous Plantar SensorDocument5 pagesCutaneous Plantar Sensoronix2000No ratings yet
- AP26Document11 pagesAP26onix2000No ratings yet
- Barré'S Vertical - E Type Global Postural UnbalanceDocument1 pageBarré'S Vertical - E Type Global Postural Unbalanceonix2000No ratings yet
- Pelvic Stabilization Hip StrengtheningDocument8 pagesPelvic Stabilization Hip StrengtheningKarlosNo ratings yet
- Barré'S Vertical - A Type Ascending Pattern With Low DysfunctionDocument1 pageBarré'S Vertical - A Type Ascending Pattern With Low Dysfunctiononix2000No ratings yet
- AP1Document8 pagesAP1onix2000No ratings yet
- Nineteenth Century Exercise Clinics For The Treatment of ScoliosisDocument7 pagesNineteenth Century Exercise Clinics For The Treatment of Scoliosisonix2000No ratings yet
- F Faculty Created Omt GustowskiDocument17 pagesF Faculty Created Omt Gustowskionix2000No ratings yet
- Sciatica Self Care BookletDocument49 pagesSciatica Self Care BookletSafetyboss100% (3)
- Lumbar Core StrenghtDocument8 pagesLumbar Core StrenghtMattia BressanNo ratings yet
- Sciatica Self Care BookletDocument49 pagesSciatica Self Care BookletSafetyboss100% (3)