You might also like
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Nursing Care PlansDocument21 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Nursing Care PlansCarl Elexer Cuyugan Ano100% (1)
- Controlling Microbial Growth in VitroDocument65 pagesControlling Microbial Growth in VitroCarl Elexer Cuyugan Ano100% (16)
- NCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNDocument1 pageNCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNCarl Elexer Cuyugan Ano100% (2)
- NCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNDocument1 pageNCP - Ineffective Airway Clearance R/T Retained Secretions 2° BPNCarl Elexer Cuyugan Ano100% (2)
- PyodermaDocument19 pagesPyodermaFajar Hidayat RamadhanNo ratings yet
- Family Case Analysis 2Document98 pagesFamily Case Analysis 2Carl Elexer Cuyugan Ano50% (2)
- NCP - Risk For Impaired Skin Integrity R/T Dry Skin and Behaviors That May Lead To Skin Integrity Impairment AEB Scratching of ScabsDocument1 pageNCP - Risk For Impaired Skin Integrity R/T Dry Skin and Behaviors That May Lead To Skin Integrity Impairment AEB Scratching of ScabsCarl Elexer Cuyugan Ano100% (4)
- Pain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalDocument50 pagesPain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalPrathiba PrassaddNo ratings yet
- AmputationDocument36 pagesAmputationaldriansilverNo ratings yet
- Cghs RatesDocument23 pagesCghs RatesVasu RathodNo ratings yet
- Rhemuatoid Arthritis: Post RN BSN 1 Semester JCON Pushpa Kumari Abdul Hafeez Raza Muhammad Ghulam Murtaza 20/11/2020Document19 pagesRhemuatoid Arthritis: Post RN BSN 1 Semester JCON Pushpa Kumari Abdul Hafeez Raza Muhammad Ghulam Murtaza 20/11/2020shewo.pirtamNo ratings yet
- Pain ScaleDocument1 pagePain Scaleyordanos getachewNo ratings yet
- Biological Basis of BehaviourDocument21 pagesBiological Basis of BehaviourSufian Khan100% (1)
- Futuristic NursingDocument14 pagesFuturistic NursingPooja JanghelNo ratings yet
- Orthopedic InjuriesDocument24 pagesOrthopedic Injuriesamber tariqNo ratings yet
- End of LifeDocument31 pagesEnd of LifeSimran JosanNo ratings yet
- The Aim of Ear, Nose and ThroatDocument32 pagesThe Aim of Ear, Nose and ThroatabdulNo ratings yet
- Fall Risk ToolDocument2 pagesFall Risk ToolannekempNo ratings yet
- Lecturer/ Magda Bayoumi: Prepared byDocument22 pagesLecturer/ Magda Bayoumi: Prepared byicrs_aamirNo ratings yet
- Lesson Plan ON AppendicitisDocument14 pagesLesson Plan ON AppendicitisrevathyNo ratings yet
- AppendicitisDocument36 pagesAppendicitisPetro MyronovNo ratings yet
- Care of Unconscious PatientDocument34 pagesCare of Unconscious PatientPoova RagavanNo ratings yet
- Evaluation Form MSCDocument5 pagesEvaluation Form MSCvikash kumarNo ratings yet
- UnconsciousnessDocument16 pagesUnconsciousnessAkhilesh BabuNo ratings yet
- 1 Pain AssessmentDocument13 pages1 Pain AssessmentQuijano GpokskieNo ratings yet
- Psychiatric EmergenciesDocument25 pagesPsychiatric EmergenciesAnnapurna DangetiNo ratings yet
- Body Posture and LiftingDocument88 pagesBody Posture and LiftingShafiq Mohd NorNo ratings yet
- Healthy LifestyleDocument29 pagesHealthy LifestyleCHRISTOPHER FAYLONNo ratings yet
- Leprosy: BY:-Sweta Upadhyay BPT 4 YearDocument29 pagesLeprosy: BY:-Sweta Upadhyay BPT 4 YearSweta upadhyayNo ratings yet
- IPRDocument20 pagesIPRAnusha VergheseNo ratings yet
- Body Mechanics - LESSON PLANDocument18 pagesBody Mechanics - LESSON PLANJincy Johny100% (1)
- Peer Group Presentation On: Recreational Therapy Play Therapy Music TherapyDocument10 pagesPeer Group Presentation On: Recreational Therapy Play Therapy Music TherapyMonikaNo ratings yet
- Preventing The Hazards of ImmobilityDocument23 pagesPreventing The Hazards of ImmobilitySUBI BABUNo ratings yet
- Neurology - : Approach To Headache DisordersDocument8 pagesNeurology - : Approach To Headache DisordersKarenNo ratings yet
- 3rd Year Internal Assessment Child Health NursingDocument20 pages3rd Year Internal Assessment Child Health NursingRajesh Kumar SahNo ratings yet
- 1 Pain Sensation Physiology DR Ambreen TauseefDocument73 pages1 Pain Sensation Physiology DR Ambreen TauseefbilalNo ratings yet
- NZONA Traction 2009Document29 pagesNZONA Traction 2009babukiranNo ratings yet
- Prolapsed Intervertebral DiscDocument12 pagesProlapsed Intervertebral DiscElvisNo ratings yet
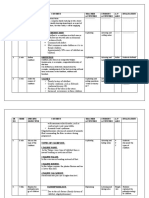
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- NCP On AppendicitisDocument7 pagesNCP On Appendicitisshweta singhNo ratings yet
- Report of Anp Icu PostingDocument5 pagesReport of Anp Icu PostingsimonjosanNo ratings yet
- Bachelor of Nursing Checklist NUR 3915 Clinical Practice V 4 (0+4)Document2 pagesBachelor of Nursing Checklist NUR 3915 Clinical Practice V 4 (0+4)Ching WeiNo ratings yet
- RestraintsDocument16 pagesRestraintsSowjanyaNo ratings yet
- Lesson Plan On Vital SignsDocument20 pagesLesson Plan On Vital SignsJincy JohnyNo ratings yet
- Colostomy CareDocument4 pagesColostomy CareRhenzes HaraNo ratings yet
- Dog BiteDocument17 pagesDog BiteSanjeev BhatiaNo ratings yet
- Psychology BSC Nursing 1St Year: Unit 1 History, Scope and Methods of PsychologyDocument17 pagesPsychology BSC Nursing 1St Year: Unit 1 History, Scope and Methods of PsychologyyashodharaNo ratings yet
- Case Report Rheumatoid ArthritisDocument29 pagesCase Report Rheumatoid ArthritisEmmy Safitri Abbas0% (1)
- Class II Neurotic DisordersDocument37 pagesClass II Neurotic DisordersNarayan K Ghorapde100% (1)
- After The Class Students Will Be Able To Gain Knowledge About TriageDocument3 pagesAfter The Class Students Will Be Able To Gain Knowledge About TriageRahul DamorNo ratings yet
- Betty NeumanDocument25 pagesBetty NeumanCarry Ann JunturaNo ratings yet
- Care of Patient With CastDocument31 pagesCare of Patient With Castيلا كورة شوت beIn sportNo ratings yet
- Burns Assessment - TeachMeSurgeryDocument5 pagesBurns Assessment - TeachMeSurgeryLaroui HoNo ratings yet
- Care of Terminally IllDocument34 pagesCare of Terminally Illbemina jaNo ratings yet
- Extended and Expanded Role of Nurse in EmergencyDocument23 pagesExtended and Expanded Role of Nurse in Emergencyankita guptaNo ratings yet
- Corneal UlcersDocument18 pagesCorneal UlcersAvinash NagarNo ratings yet
- Pain and Pain ManagementDocument7 pagesPain and Pain ManagementNatukunda DianahNo ratings yet
- Anaphylactic ShockDocument11 pagesAnaphylactic ShockBushra NaeemNo ratings yet
- Unit - I IntroConcepts of Psychiatric NursingDocument16 pagesUnit - I IntroConcepts of Psychiatric NursingNarayan K GhorapdeNo ratings yet
- Patient EnvironmentDocument34 pagesPatient EnvironmentSILUVERU SALOMINo ratings yet
- PainDocument20 pagesPainvinnu kalyanNo ratings yet
- UnconsciousnessDocument15 pagesUnconsciousnesssippuNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Sweet’s Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSweet’s Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- (Ha Lab) Sas#9Document9 pages(Ha Lab) Sas#9Erwin RomeroNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- Ectopic Pregnancy Study GuideDocument5 pagesEctopic Pregnancy Study GuideCarl Elexer Cuyugan Ano100% (1)
- Iii. Patient and His Illness A. Review of Anatomy and PhysiologyDocument13 pagesIii. Patient and His Illness A. Review of Anatomy and PhysiologyCarl Elexer Cuyugan AnoNo ratings yet
- CarlncmDocument2 pagesCarlncmCarl Elexer Cuyugan AnoNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" IntroDocument6 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" IntroCarl Elexer Cuyugan AnoNo ratings yet
- Craniotomy Surgical Case ReportDocument58 pagesCraniotomy Surgical Case ReportCarl Elexer Cuyugan Ano100% (9)
- Nurse0710 PampangaDocument135 pagesNurse0710 PampangaproffsgNo ratings yet
- Hypertension Study GuideDocument4 pagesHypertension Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- Hydatidiform Mole Study GuideDocument4 pagesHydatidiform Mole Study GuideCarl Elexer Cuyugan AnoNo ratings yet
- B. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelDocument2 pagesB. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelCarl Elexer Cuyugan Ano50% (2)
- Traumatic Brain Injuries Study GuideDocument18 pagesTraumatic Brain Injuries Study GuideCarl Elexer Cuyugan Ano100% (1)
- Diversity of Microorganisms 2Document71 pagesDiversity of Microorganisms 2Carl Elexer Cuyugan Ano100% (4)
- Microbial Physiology and Genetics Part 1Document43 pagesMicrobial Physiology and Genetics Part 1Carl Elexer Cuyugan Ano100% (7)
- Neonatal Sepsis (Sepsis Neonatorum) Medical Management Not Included...Document29 pagesNeonatal Sepsis (Sepsis Neonatorum) Medical Management Not Included...Carl Elexer Cuyugan Ano100% (3)
- Principles of Antimicrobial Therapy Part 1Document83 pagesPrinciples of Antimicrobial Therapy Part 1Carl Elexer Cuyugan Ano100% (1)
- Diversity of Microorganisms 1 - AcellularDocument39 pagesDiversity of Microorganisms 1 - AcellularCarl Elexer Cuyugan Ano100% (1)
- Diversity of Microorganisms 1 - ProkaryoticDocument45 pagesDiversity of Microorganisms 1 - ProkaryoticCarl Elexer Cuyugan Ano100% (6)
- Shapes and Arrangements of BacteriaDocument22 pagesShapes and Arrangements of BacteriaCarl Elexer Cuyugan Ano100% (3)
- The Metabolic and Endocrine Systems NotesDocument9 pagesThe Metabolic and Endocrine Systems NotesCarl Elexer Cuyugan Ano100% (2)
- Cell Structure and TaxonomyDocument50 pagesCell Structure and TaxonomyCarl Elexer Cuyugan AnoNo ratings yet
- Basic Drug Computations Part 1Document8 pagesBasic Drug Computations Part 1Carl Elexer Cuyugan Ano100% (4)
- Gastrointestinal Tract System NotesDocument8 pagesGastrointestinal Tract System NotesCarl Elexer Cuyugan Ano100% (1)
- Complications of Intravenous TherapyDocument37 pagesComplications of Intravenous TherapyCarl Elexer Cuyugan Ano100% (3)
- Basic Computations 2 IV & IVFDocument37 pagesBasic Computations 2 IV & IVFCarl Elexer Cuyugan Ano100% (5)