You might also like
- Tesco Bank - No Claim Discount 28.11.17Document2 pagesTesco Bank - No Claim Discount 28.11.17eujenio50% (2)
- NCEA Numeracy Sample Common Assessment ActivityDocument16 pagesNCEA Numeracy Sample Common Assessment ActivityStuff Newsroom20% (5)
- Tom Houggard MergedDocument269 pagesTom Houggard MergedTomojeet Chakraborty100% (2)
- Nursing Care Plan Fluid Volume DeficitDocument2 pagesNursing Care Plan Fluid Volume DeficitXtinego89% (9)
- NCP Pediatric (Diarrhea and Impaired Mucous Membrane)Document8 pagesNCP Pediatric (Diarrhea and Impaired Mucous Membrane)Flauros Ryu Jabien60% (5)
- NCP Risk For Fluid Volume DeficitDocument2 pagesNCP Risk For Fluid Volume DeficitJeanineReyes44% (9)
- NCP Fluid Volume DeficitDocument2 pagesNCP Fluid Volume DeficitRez Apego0% (1)
- NCP Impaired Gas ExchangeDocument4 pagesNCP Impaired Gas ExchangeKen Simon100% (1)
- NCPs For Diabetes MellitusDocument6 pagesNCPs For Diabetes MellitusEjie Boy Isaga100% (1)
- Diarrhea NCPDocument3 pagesDiarrhea NCPCharles Michael Azagra0% (1)
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- JVJV NCP Risk For Fluid Volume DeficitDocument2 pagesJVJV NCP Risk For Fluid Volume DeficitvicenteturasNo ratings yet
- NCP For Deficient Fluid VolumeDocument2 pagesNCP For Deficient Fluid VolumeRedwing_Dc_854758% (12)
- NCP. Deficient Fluid Volume by Eben D.C.Document1 pageNCP. Deficient Fluid Volume by Eben D.C.dominoredwing2024100% (1)
- Fluid Volume Deficit BatuDocument2 pagesFluid Volume Deficit Batumecz26No ratings yet
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- NCP Deficient Fluid Volume Related To Fluid Loss DHNDocument2 pagesNCP Deficient Fluid Volume Related To Fluid Loss DHNMa. Elaine Carla Tating38% (8)
- Risk For Deficient Fluid Volume - NCPDocument2 pagesRisk For Deficient Fluid Volume - NCPAyla Mar100% (1)
- Assessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKSDocument3 pagesAssessment Healt H Patte RN Nursing Diagnosis Desired Outcome (Edit) Intervention (Edit) Evaluation (EDIT) Rema RKStflorenzNo ratings yet
- NCP-Deficient Fluid VolumeDocument1 pageNCP-Deficient Fluid Volumejanmichael8No ratings yet
- NCP HyperthermiaDocument6 pagesNCP HyperthermiaGrax DeeNo ratings yet
- Short Term: Independent: Independent: Short TermDocument2 pagesShort Term: Independent: Independent: Short TermAndre ImperialNo ratings yet
- NCP DiarrheaDocument2 pagesNCP DiarrheaMiguelMartinNo ratings yet
- Electrolyte Imbalance NCPDocument8 pagesElectrolyte Imbalance NCPManuel Jacob YradNo ratings yet
- NCPDocument4 pagesNCPAndrea BroccoliNo ratings yet
- Fluid Volume DeficitDocument2 pagesFluid Volume DeficitRuby AnneNo ratings yet
- Impaired Gas Exchange NCPDocument4 pagesImpaired Gas Exchange NCPkimglaidyl bontuyanNo ratings yet
- NCP (Deficient Fluid VolumeDocument3 pagesNCP (Deficient Fluid VolumeNica RespondoNo ratings yet
- NCP - Diarrhea - FeunrmfDocument7 pagesNCP - Diarrhea - FeunrmfJk SalvadorNo ratings yet
- NCP Ineffective Airway Clearance Related To The Accumulation of Exudates in The Alveoli TBDocument3 pagesNCP Ineffective Airway Clearance Related To The Accumulation of Exudates in The Alveoli TBMa. Elaine Carla Tating0% (1)
- Fluid Volume DeficitDocument3 pagesFluid Volume Deficitprickybiik100% (1)
- NCP For Ineffective Breathing Pattern - RMC CasepressDocument2 pagesNCP For Ineffective Breathing Pattern - RMC Casepressmissyuri08No ratings yet
- Impaired Gas Exchange NCPDocument1 pageImpaired Gas Exchange NCPCj AlconabaNo ratings yet
- NCP GastroenteritisDocument1 pageNCP GastroenteritisFranchesca PaunganNo ratings yet
- NCPDocument9 pagesNCPYesha Mae MartinNo ratings yet
- Hyperthermia NCPDocument2 pagesHyperthermia NCPSian AsadaNo ratings yet
- NCP FVDDocument2 pagesNCP FVDMarlon AnryNo ratings yet
- Ineffective Breathing PatternDocument8 pagesIneffective Breathing PatternJansen Arquilita Rivera100% (2)
- NCPDocument6 pagesNCPKyla Carbonel100% (1)
- Ineffective Tissue PerfusionDocument4 pagesIneffective Tissue PerfusionClariz Basco100% (1)
- HyperthermiaDocument6 pagesHyperthermiaBerlyn FelicianoNo ratings yet
- NCP - HyperthermiaDocument3 pagesNCP - Hyperthermiaedmr12No ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument7 pagesCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisNo ratings yet
- NCP-Risk For Fluid Volume DeficitDocument3 pagesNCP-Risk For Fluid Volume DeficitJai Go100% (1)
- NCP DiarrheaDocument2 pagesNCP DiarrheaBracel GarciaNo ratings yet
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- Body Weakness NCPDocument1 pageBody Weakness NCPtwicetrashNo ratings yet
- Deficit)Document2 pagesDeficit)Lee DeeNo ratings yet
- NCP DengueDocument3 pagesNCP DenguejhaninahNo ratings yet
- Nursing Care Plan: IndependentDocument2 pagesNursing Care Plan: IndependentAdhaNo ratings yet
- Disturbed SleepDocument1 pageDisturbed Sleepmawel100% (1)
- Daily NCPDocument5 pagesDaily NCPKuennie SabalNo ratings yet
- Diarrhea NCPDocument3 pagesDiarrhea NCPCharles Michael AzagraNo ratings yet
- NCP - ConstipationDocument3 pagesNCP - ConstipationDaniel Dave KapunanNo ratings yet
- Volume 1Document2 pagesVolume 1roxybiscanteNo ratings yet
- Prado NCPDocument4 pagesPrado NCPalleah pradoNo ratings yet
- Acute Poststreptoccal GlumerulonephritisDocument3 pagesAcute Poststreptoccal GlumerulonephritisElle RosalesNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationpamelaideaNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiNo ratings yet
- CholeraDocument3 pagesCholeraKrista CabelloNo ratings yet
- Case Study: Subjective: Objective: General Objective: Independent IndependentDocument10 pagesCase Study: Subjective: Objective: General Objective: Independent IndependentChristine EmanNo ratings yet
- Salva, R.D NCP & Drug Study (Isph - Gs Pediaward)Document7 pagesSalva, R.D NCP & Drug Study (Isph - Gs Pediaward)Rae Dominick Aquino SalvaNo ratings yet
- Nursing Care Plan For DM PatientDocument10 pagesNursing Care Plan For DM PatientRainier Rhett Concha100% (5)
- Lesson PlanDocument6 pagesLesson Plannurulhuda287No ratings yet
- Million Dollar Theft Sol 2015Document3 pagesMillion Dollar Theft Sol 2015KeremNo ratings yet
- CJHP 66 369Document6 pagesCJHP 66 369lia pramudha wardhaniNo ratings yet
- Transmisores Foxboro-NeumaticosDocument12 pagesTransmisores Foxboro-Neumaticoscampana02No ratings yet
- Literature Component Captain Nobody English SPM PDFDocument11 pagesLiterature Component Captain Nobody English SPM PDFmeshal retteryNo ratings yet
- David Howes The Craft of The SensesDocument9 pagesDavid Howes The Craft of The SensesMehdi FaizyNo ratings yet
- GLS340 - LP Report EngineDocument10 pagesGLS340 - LP Report EngineNurul IzzahNo ratings yet
- Dari SiniDocument7 pagesDari SinidindasaviraNo ratings yet
- Journey MGT Plan (Land)Document14 pagesJourney MGT Plan (Land)nelson ogidiNo ratings yet
- Syllabus - Momentum Transfer Lec and LabDocument6 pagesSyllabus - Momentum Transfer Lec and LabKzenetteNo ratings yet
- Rurban PowerPoint Presentation Final OneDocument65 pagesRurban PowerPoint Presentation Final OneVIVEK VERMANo ratings yet
- The Science Behind Skin Care: Cleansers: Zoe Diana Draelos MDDocument7 pagesThe Science Behind Skin Care: Cleansers: Zoe Diana Draelos MDkinayungNo ratings yet
- Mucoadhesive DDS - 1749098145Document14 pagesMucoadhesive DDS - 1749098145Vaibhav ThoratNo ratings yet
- Fixed DepositsDocument1 pageFixed DepositsTiso Blackstar GroupNo ratings yet
- Re5r05a 2Document18 pagesRe5r05a 2Denis KonovalovNo ratings yet
- Yarn Over 101Document3 pagesYarn Over 101Bea Ann83% (6)
- Dip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Document1 pageDip Obst (SA) Past Papers - 2020 1st Semester 1-6-2023Neo Latoya MadunaNo ratings yet
- Channel Estimation Using SVR - REPORTDocument33 pagesChannel Estimation Using SVR - REPORTVighnesh S BhatNo ratings yet
- 2008 - Aecom - UK AirportTerminals - CM - 1aug08Document6 pages2008 - Aecom - UK AirportTerminals - CM - 1aug08Yi JieNo ratings yet
- Fractured Root Tips During Dental Extractions and Retained Root Fragments. A Clinical Dilemma?Document7 pagesFractured Root Tips During Dental Extractions and Retained Root Fragments. A Clinical Dilemma?Siti Ulfah NesiaNo ratings yet
- Sawatdee Hello Beautiful BangkokDocument20 pagesSawatdee Hello Beautiful BangkokRhea RedulfaNo ratings yet
- Wande Coal - Mushin 2 Mo HitsDocument3 pagesWande Coal - Mushin 2 Mo HitsOye Akideinde100% (2)
- A Teacher's DiaryDocument5 pagesA Teacher's DiaryJoreene CedroNo ratings yet
- ZvsDocument22 pagesZvsgopalchandramahatoNo ratings yet
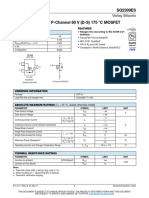
- Sq2309es RB VishayDocument12 pagesSq2309es RB VishayBenjaminNo ratings yet
- Danik Bhaskar Jaipur 07-02-2014Document26 pagesDanik Bhaskar Jaipur 07-02-2014bhaskar_newsNo ratings yet
- Handbook of Spectrum Monitoring 2011Document678 pagesHandbook of Spectrum Monitoring 2011haripost100% (1)