You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- LDN Letter To Give To Your DoctorDocument3 pagesLDN Letter To Give To Your DoctorbktangoNo ratings yet
- Burton's Microbiology For The Health Sciences: Diagnosing Infectious DiseasesDocument35 pagesBurton's Microbiology For The Health Sciences: Diagnosing Infectious DiseasesJehu C LanieNo ratings yet
- LDN Information (2!19!17 Update)Document18 pagesLDN Information (2!19!17 Update)bktango100% (1)
- Important LDN NOTES (7.22.2012 Update)Document20 pagesImportant LDN NOTES (7.22.2012 Update)bktangoNo ratings yet
- Important LDN Notes: Author: Diana GaleDocument22 pagesImportant LDN Notes: Author: Diana GalebktangoNo ratings yet
- The Faces of Low Dose NaltrexoneDocument116 pagesThe Faces of Low Dose Naltrexonebktango100% (1)
- Google LDN (E-Book)Document146 pagesGoogle LDN (E-Book)bktangoNo ratings yet
- 201 Reasons For LDNDocument386 pages201 Reasons For LDNbktango100% (2)
- Menerapkan Keselamatan, Kesehatan Kerja (k3) Dan HygineDocument22 pagesMenerapkan Keselamatan, Kesehatan Kerja (k3) Dan HygineagumsyahNo ratings yet
- Leukaemia PDFDocument21 pagesLeukaemia PDFbrijsingNo ratings yet
- High Power Committee On Nursing in India - Doc 2003Document10 pagesHigh Power Committee On Nursing in India - Doc 2003Sujatha J JayabalNo ratings yet
- The Complete Anti-Inflammatory Diet For Beginners: A No-Stress Meal Plan With Easy Recipes To Heal The Immune SystemDocument4 pagesThe Complete Anti-Inflammatory Diet For Beginners: A No-Stress Meal Plan With Easy Recipes To Heal The Immune SystemNina Foreel0% (3)
- Nursing TheoriesDocument13 pagesNursing TheoriesIrfan-ullah Ik KhanNo ratings yet
- WEEK 2 - 1 - Introduction of PathologyDocument20 pagesWEEK 2 - 1 - Introduction of Pathologyotaibynaif100% (1)
- Code Blue PDFDocument9 pagesCode Blue PDFanggristyanugrohoNo ratings yet
- DoxycyclineDocument18 pagesDoxycyclineSabab MunifNo ratings yet
- Grief and Loss Answer-7Document3 pagesGrief and Loss Answer-7June DumdumayaNo ratings yet
- Distinguish The Basic Terms in Special Education From Each OtherDocument2 pagesDistinguish The Basic Terms in Special Education From Each OtherMARICRIS LLANONo ratings yet
- Blood Bank Information SystemDocument63 pagesBlood Bank Information SystemSaravanan RajagopalNo ratings yet
- Format Compact Case Loads UPCNDocument5 pagesFormat Compact Case Loads UPCNPaul Christian P. Santos, RNNo ratings yet
- Dimethyl FumarateDocument2 pagesDimethyl FumarateAbrar AlNabhanNo ratings yet
- Penyakit Menular SeksualDocument83 pagesPenyakit Menular SeksualIvan Ho0% (1)
- Technical Notes Community Health NursingDocument8 pagesTechnical Notes Community Health NursingMary JoyNo ratings yet
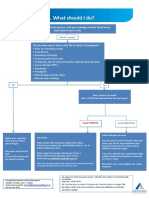
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Literature ReviewDocument8 pagesLiterature Reviewapi-268670617No ratings yet
- Cad Cam International2 2016all PDFDocument52 pagesCad Cam International2 2016all PDFDragoş Şerban PopNo ratings yet
- MalnutritionDocument27 pagesMalnutritionRIYA MARIYATNo ratings yet
- Ai in Healthcare 202011 201117103639Document17 pagesAi in Healthcare 202011 201117103639羅浩維No ratings yet
- Raw For Life - Free Interview Series - Hosted by Drs. Rick and Karin Dina - Raw For Life Summit - HTMLDocument6 pagesRaw For Life - Free Interview Series - Hosted by Drs. Rick and Karin Dina - Raw For Life Summit - HTMLelissaios0% (1)
- Assoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivDocument106 pagesAssoc. Prof. G. Tomov, PHD: Division of Oral Pathology, Faculty of Dental Medicine Mu - PlovdivAustine OsaweNo ratings yet
- Ujjol MainDocument6 pagesUjjol MaintashfimmironNo ratings yet
- National Drug PolicyDocument17 pagesNational Drug PolicyKhadija KamranNo ratings yet
- Memmory Shit 1 2 1Document3 pagesMemmory Shit 1 2 1Cristian Radu100% (1)
- Musculoskeletal EmergenciesDocument548 pagesMusculoskeletal Emergenciesjomalu210377No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument18 pagesChronic Obstructive Pulmonary DiseaseMaryam BajwaNo ratings yet
- Faculy of Computer Science and Engineering Project Registration Form Final Year Project YEARDocument1 pageFaculy of Computer Science and Engineering Project Registration Form Final Year Project YEARSadiq Shah Yushi BazukayNo ratings yet
- Hormonal Imbalance and Its Causes in Young Females: January 2015Document6 pagesHormonal Imbalance and Its Causes in Young Females: January 2015figgernaggotNo ratings yet