You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Appendix Chapter, Sabiston Textbook of SurgeryDocument43 pagesAppendix Chapter, Sabiston Textbook of SurgeryShuo Huang100% (2)
- Problem Nursing Diagnosis Outcome Plan Intervention Evaluation Subjective Data: "Masakit Po Yung Sa Short Term: IndependentDocument2 pagesProblem Nursing Diagnosis Outcome Plan Intervention Evaluation Subjective Data: "Masakit Po Yung Sa Short Term: IndependentkyawNo ratings yet
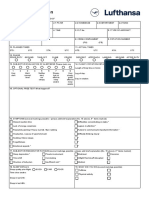
- Lufthansa Fatigue Call ReportDocument1 pageLufthansa Fatigue Call ReportMOHIT GOYALNo ratings yet
- Deaths Web Report Suppl Tables 1Document101 pagesDeaths Web Report Suppl Tables 1Giorno GiovannaNo ratings yet
- Conjunctivitis - PinkeyeDocument3 pagesConjunctivitis - PinkeyeJenna HenryNo ratings yet
- Presentstion No-1Document15 pagesPresentstion No-1Lally LukeNo ratings yet
- GeneticsDocument75 pagesGeneticsDema AbunnadiNo ratings yet
- Performance Enhancing DrugsDocument18 pagesPerformance Enhancing Drugsapi-594103526No ratings yet
- GorantlaDocument18 pagesGorantlaapi-464986748No ratings yet
- VIRAL MENINGITIS John GreenDocument3 pagesVIRAL MENINGITIS John Greenbradle2005No ratings yet
- Anaphylaxis Diagnosis and ManagementDocument10 pagesAnaphylaxis Diagnosis and Managementd dNo ratings yet
- NCM 116 - Medical Surgical Nursing Lecture 01/26/2023: Spiritual CareDocument6 pagesNCM 116 - Medical Surgical Nursing Lecture 01/26/2023: Spiritual CareIvan A. EleginoNo ratings yet
- Diadens PC ManualDocument31 pagesDiadens PC Manualvdbroger100% (1)
- WIDGB4 AK Utest Language 6Document4 pagesWIDGB4 AK Utest Language 6mintymouse881No ratings yet
- Sudden Visual Loss - PPTX, EmergencyDocument31 pagesSudden Visual Loss - PPTX, EmergencydesmyyNo ratings yet
- 401H Report BioHealth 7 16 PDFDocument1 page401H Report BioHealth 7 16 PDFgreatgeniusNo ratings yet
- Bino - Lec - Midterm Exam - Yellow - PadDocument11 pagesBino - Lec - Midterm Exam - Yellow - PadDanielle SangalangNo ratings yet
- Male Pelvic Organ 1Document73 pagesMale Pelvic Organ 1Juhar AhamedNo ratings yet
- Homœopathic Materia MedicaDocument193 pagesHomœopathic Materia MedicaMohammad ShoebNo ratings yet
- Hemolytic Anemia SDocument1 pageHemolytic Anemia Sdnutter012576No ratings yet
- Should I Stop Being A Perfectionist?Document3 pagesShould I Stop Being A Perfectionist?Maia GroisNo ratings yet
- Simple EmergenciesDocument177 pagesSimple Emergenciesharsh89100% (1)
- Intestinal Diseases in Cattle 2023Document30 pagesIntestinal Diseases in Cattle 2023Krystyna WędrychowskaNo ratings yet
- Kaileigh Sweeney, SN University of Rhode Island Mentor: Carolyn HamesDocument30 pagesKaileigh Sweeney, SN University of Rhode Island Mentor: Carolyn HamesJulie Marie PavadoraNo ratings yet
- VertigoDocument4 pagesVertigoshedNo ratings yet
- Roberto Rodriguez-Ruesga MD FACS FASCRSDocument2 pagesRoberto Rodriguez-Ruesga MD FACS FASCRSyadneshbachaNo ratings yet
- Wilkins Clinical Assessment in Respiratory Care 7th Edition by Heuer - Test BankDocument37 pagesWilkins Clinical Assessment in Respiratory Care 7th Edition by Heuer - Test BankalishcathrinNo ratings yet
- Respiratory Distress SyndromeDocument54 pagesRespiratory Distress SyndromeKristine CaringalNo ratings yet
- Hepatic Cysts Workup: Approach ConsiderationsDocument4 pagesHepatic Cysts Workup: Approach ConsiderationsMariska JuanitaNo ratings yet
- Axelsson 1978Document7 pagesAxelsson 1978Andreea CiorneaNo ratings yet