You might also like
- CirrhosisDocument54 pagesCirrhosisYani88% (8)
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- Gi BleedDocument28 pagesGi BleedligitafitranandaNo ratings yet
- Gastrointestinal Bleeding: PCOM Internal Medicine Residents 2004Document30 pagesGastrointestinal Bleeding: PCOM Internal Medicine Residents 2004nesakusumaNo ratings yet
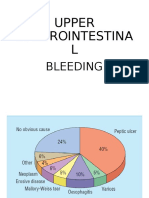
- Upper Gi BleedingDocument36 pagesUpper Gi BleedingHalimatul SaadiahNo ratings yet
- Gastrointestinal AlterationsDocument40 pagesGastrointestinal AlterationsMajesty ParkerNo ratings yet
- Upper Gastrointestina L: BleedingDocument35 pagesUpper Gastrointestina L: BleedingayuNo ratings yet
- Gastrointestinal Disorders: CPT Donald C Palma MCDocument28 pagesGastrointestinal Disorders: CPT Donald C Palma MCJorge RabajaNo ratings yet
- Symptoms and Signs in Acute Abdominal PainDocument40 pagesSymptoms and Signs in Acute Abdominal PainPoh TseNo ratings yet
- Obstructive Jaundice 2020Document4 pagesObstructive Jaundice 2020Choden JamyangNo ratings yet
- Edema: Leyi Gu Renal Division, Renji HospitalDocument27 pagesEdema: Leyi Gu Renal Division, Renji HospitalIdham BaharudinNo ratings yet
- Gi BleedDocument33 pagesGi BleedMuhammad ArmghanNo ratings yet
- Upper Gi BleedDocument47 pagesUpper Gi BleedAtul SharmaNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibJohn Clements Galiza100% (1)
- Liver Cirrhosis: DR Alex MogereDocument51 pagesLiver Cirrhosis: DR Alex MogereGladys Maina100% (1)
- Fluid Volume DisturbancesDocument25 pagesFluid Volume Disturbancesmoonlight ariNo ratings yet
- GI Bleeding:: From Mouth To RectumDocument31 pagesGI Bleeding:: From Mouth To RectumBendy Dwi IrawanNo ratings yet
- UremiaDocument52 pagesUremiamgopigio5No ratings yet
- Jaundice: DremsaidDocument42 pagesJaundice: DremsaidabdallhNo ratings yet
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilNo ratings yet
- Gastrointestinal Bleeding in NewbornDocument28 pagesGastrointestinal Bleeding in NewbornHafiz AwaisNo ratings yet
- Fluid Electrolytes 2Document22 pagesFluid Electrolytes 2QueenClerk VillarteNo ratings yet
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibdiaNo ratings yet
- Approach To A Patient With Upper GI BleedDocument42 pagesApproach To A Patient With Upper GI BleedMuhammad Naveed AslamNo ratings yet
- Acute and Chronic Liver Disease - Orla CrosbieDocument46 pagesAcute and Chronic Liver Disease - Orla CrosbiewasimqureshiNo ratings yet
- Student Copy of Gastrointestinal Problems SP 2010 IggyDocument80 pagesStudent Copy of Gastrointestinal Problems SP 2010 IggyJade CentinoNo ratings yet
- Atul Sharma Uppergi Fcccm23Document47 pagesAtul Sharma Uppergi Fcccm23Atul SharmaNo ratings yet
- CPC Edit RMDocument39 pagesCPC Edit RMSoumya GuptaNo ratings yet
- GerdDocument43 pagesGerdNidhi shriNo ratings yet
- Acute Chronic Kidney InjuryDocument29 pagesAcute Chronic Kidney InjuryPriya GKNo ratings yet
- 1100 Ultrasound of The Acute Abdomen 15 3Document84 pages1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016No ratings yet
- Middle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDDocument66 pagesMiddle Age Man With Nephrotic Syndrome, Ascitis and Edema: Raika Jamali MDyusnafratilova16No ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- New Upper Gi BleedDocument35 pagesNew Upper Gi Bleedapi-195799092No ratings yet
- Liver CirhosisDocument72 pagesLiver CirhosisamadoorahmedNo ratings yet
- PembahasanDocument1,129 pagesPembahasanatc100% (1)
- EdemaDocument27 pagesEdemaAyyappan JayavelNo ratings yet
- Esophageal Varices AMJDocument35 pagesEsophageal Varices AMJAli Al.JuffairiNo ratings yet
- Portal Hypertension: Dr. Ravi Gadani MS, FmasDocument57 pagesPortal Hypertension: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- CIRRHOSIS v1Document41 pagesCIRRHOSIS v1anil sahNo ratings yet
- 01 - Signs and Symptoms of Git DisordersDocument51 pages01 - Signs and Symptoms of Git DisordersRere AnugrahNo ratings yet
- UgumDocument50 pagesUgumhailu henockNo ratings yet
- EdemaDocument27 pagesEdemarapadilNo ratings yet
- Acute PancreatitisDocument60 pagesAcute PancreatitisHara TsolakidouNo ratings yet
- Intussusception: DR Phillipo Leo ChalyaDocument19 pagesIntussusception: DR Phillipo Leo ChalyaSibabaong'ombe MasakaNo ratings yet
- Abdominal Distention and AscitesDocument49 pagesAbdominal Distention and AscitesNinaNo ratings yet
- Managing Common Ward CallsDocument55 pagesManaging Common Ward CallsShuvashis TituNo ratings yet
- Acute Renal Failure Chronic Renal FailureDocument48 pagesAcute Renal Failure Chronic Renal Failurekimchi girlNo ratings yet
- Budd Chiari Syndrome: by DR - Kamran M SaeedDocument41 pagesBudd Chiari Syndrome: by DR - Kamran M SaeeddockmsNo ratings yet
- Upper Gi BleedingDocument37 pagesUpper Gi Bleedingfathima AlfasNo ratings yet
- C5. Renal Disorders (Nephrotic S. - Renal F.)Document44 pagesC5. Renal Disorders (Nephrotic S. - Renal F.)coco brillqnteNo ratings yet
- Perdarahan Saluran CernaDocument21 pagesPerdarahan Saluran CernaAmalia Hendar PangestutiNo ratings yet
- CKD Case PresentationDocument25 pagesCKD Case PresentationMohamed Anwer NaleefNo ratings yet
- Renal NotesDocument11 pagesRenal NotesPatty Pasarilla Passehl100% (2)
- Hepatic Venous Disease 2Document22 pagesHepatic Venous Disease 2Self UpgradeNo ratings yet
- Hematemesis Melena (Upper Gi Bleeding)Document134 pagesHematemesis Melena (Upper Gi Bleeding)Mardoni Efrijon100% (1)
- Upper GI Bleed - SymposiumDocument38 pagesUpper GI Bleed - SymposiumSopna ZenithNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- Ischemic Stroke in Young AdultDocument26 pagesIschemic Stroke in Young AdultBill Jones TanawalNo ratings yet
- TextbookofRogaNidanaandVikritiVIgyanDr Gopikrishnas AcharyaDocument72 pagesTextbookofRogaNidanaandVikritiVIgyanDr Gopikrishnas AcharyaArunakumar CNo ratings yet
- Clarithromycin Drug StudyDocument1 pageClarithromycin Drug StudyDivine LavaNo ratings yet
- 14 CefaleeaDocument52 pages14 Cefaleeagabriela.nicolescuNo ratings yet
- Tibia FracturesDocument15 pagesTibia FracturesmoimoimoibaridacheNo ratings yet
- Interpretation of Urine CulturesDocument29 pagesInterpretation of Urine Culturestummalapalli venkateswara raoNo ratings yet
- Nursing Care Plan For Pulmonary Edema PDFDocument2 pagesNursing Care Plan For Pulmonary Edema PDFAsmaa100% (1)
- Inflammatory Bowel Disease (Ibd)Document3 pagesInflammatory Bowel Disease (Ibd)Muhammad Ahmad RazaNo ratings yet
- Pierre Robin Syndrome A Case ReportDocument2 pagesPierre Robin Syndrome A Case ReportResearch ParkNo ratings yet
- Frozen Shoulder Causes and TreatmentsDocument11 pagesFrozen Shoulder Causes and TreatmentsSylvia GraceNo ratings yet
- Ear HematomaDocument3 pagesEar HematomaSafeer GhalibNo ratings yet
- Crigler-Najjar Syndrome - UpToDateDocument31 pagesCrigler-Najjar Syndrome - UpToDateMihaela Alexandra RepeziNo ratings yet
- 1.6+7 Laboratory Investigation and Film Interpretation WITHOUT ANSWERSDocument21 pages1.6+7 Laboratory Investigation and Film Interpretation WITHOUT ANSWERSAlex KamougerosNo ratings yet
- PAROS (Case 3)Document2 pagesPAROS (Case 3)Carl Michael RazoNo ratings yet
- Gridhrasi Case PresentationDocument35 pagesGridhrasi Case PresentationAmogha Kulkarni100% (1)
- Wiki - Week 1 - The Nervous System - CourseraDocument3 pagesWiki - Week 1 - The Nervous System - Courseracharles luisNo ratings yet
- NATVNS Paediatric Glamorgan v7Document5 pagesNATVNS Paediatric Glamorgan v7Nie AfnyNo ratings yet
- Typhoid Fever: Infectious DiseaseDocument52 pagesTyphoid Fever: Infectious Disease12. Akshit AtwalNo ratings yet
- 65 - Approach To Patients With CancerDocument1 page65 - Approach To Patients With CancerRica Alyssa PepitoNo ratings yet
- Heart Transplantation: Dr. K V Siva KrishnaDocument133 pagesHeart Transplantation: Dr. K V Siva KrishnaRahul K. JagaNo ratings yet
- LP Tumor Mamae OkDocument13 pagesLP Tumor Mamae OkDiban namiNo ratings yet
- Prof. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversiDocument35 pagesProf. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversidrroytambunanNo ratings yet
- Diskusi Topik 2 (PPOK) - Nafisa Zulpa Elhapidi - 406202067Document59 pagesDiskusi Topik 2 (PPOK) - Nafisa Zulpa Elhapidi - 406202067nafisa zulfaelNo ratings yet
- Cataract - GlaucomaDocument2 pagesCataract - GlaucomaggukNo ratings yet
- 4 Pharma General AnestheticsDocument10 pages4 Pharma General AnestheticsisahNo ratings yet
- Froelich Syndrome and HomoeopathyDocument13 pagesFroelich Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- CNS DR Najeeb Notes Part 3Document3 pagesCNS DR Najeeb Notes Part 3Dr. Tarush DhawanNo ratings yet
- Kawasaki Disease: An Update: EpidemiologyDocument10 pagesKawasaki Disease: An Update: EpidemiologyEmma González de BaideNo ratings yet
- NZ Crisis Handbook - DiagnosingDocument16 pagesNZ Crisis Handbook - DiagnosingSean SmythNo ratings yet
- Botulism As A Bioterrorism AgentDocument24 pagesBotulism As A Bioterrorism AgentFabián FernándezNo ratings yet