You might also like
- Wound Assessment ChartDocument2 pagesWound Assessment ChartAnonymous H3DpmCZX100% (6)
- Insulin Wall ChartDocument1 pageInsulin Wall Charturcrony10No ratings yet
- Stroke Topic DiscussionDocument19 pagesStroke Topic Discussionapi-648714317No ratings yet
- Ethical and Legal Issues in Perioperative NursingDocument3 pagesEthical and Legal Issues in Perioperative NursingJohn Pearl Fernandez100% (2)
- PFK BisoprololDocument10 pagesPFK BisoprololFelicia Aurelia SurbaktiNo ratings yet
- Idoxuridine 0.5% Ophthalmic OintmentDocument1 pageIdoxuridine 0.5% Ophthalmic Ointmentmd_corona62No ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- Obat Anti HipertensiDocument9 pagesObat Anti Hipertensisilvanus giovannyNo ratings yet
- Algoritma Nyeri Dada - Dian WDocument4 pagesAlgoritma Nyeri Dada - Dian WfaberNo ratings yet
- Metamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical ProfileDocument16 pagesMetamizole A Review Profile of A Well Known Forgotten Drug Part II Clinical ProfileTifanny WijayaNo ratings yet
- Maccura Laboratories New Test Slides Rene PDFDocument4 pagesMaccura Laboratories New Test Slides Rene PDFRicardo NinaNo ratings yet
- Contoh Jurnal Case ControlDocument7 pagesContoh Jurnal Case Controlkrisnantara7No ratings yet
- Medicinus JournalDocument68 pagesMedicinus JournalDian Rosdiani FajrinNo ratings yet
- Obat Obat HipertensiDocument74 pagesObat Obat HipertensiIlham Habib DjarkoniNo ratings yet
- Antagonis AdrenergikDocument34 pagesAntagonis AdrenergikGde Ananda ArmanditaNo ratings yet
- 2319Document4 pages2319Iqha HoNeysweetNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- Guideline Stroke Perdossi 2007Document15 pagesGuideline Stroke Perdossi 2007Saut 'tetZ' PurbaNo ratings yet
- Infectous DiseaseDocument9 pagesInfectous DiseasejamikawasNo ratings yet
- Adverse Drug ReactionDocument4 pagesAdverse Drug ReactionRahmatulloh Al HusnaNo ratings yet
- Drug Related ProblemDocument13 pagesDrug Related ProblemLinda Yuni LestariNo ratings yet
- Konsensus DM Perkeni 2006 PDFDocument55 pagesKonsensus DM Perkeni 2006 PDFDenny LukasNo ratings yet
- Dr. Widyati ADR ANALYSIS-PERSIDocument39 pagesDr. Widyati ADR ANALYSIS-PERSIHanaNo ratings yet
- Kumpulan Jurnal MedicinusDocument48 pagesKumpulan Jurnal MedicinusFatikhatul BaruniNo ratings yet
- Price List Spectra - Update 8 Juni 2023Document11 pagesPrice List Spectra - Update 8 Juni 2023Eko PrasetyoNo ratings yet
- Drug Utilization Study (Dus)Document17 pagesDrug Utilization Study (Dus)Arif Budiman100% (1)
- Diagnostik Dan Tatalaksana Stable CAD - CCSDocument38 pagesDiagnostik Dan Tatalaksana Stable CAD - CCSIno HajrinNo ratings yet
- Tia Abcd2 Tool 1Document2 pagesTia Abcd2 Tool 1Siti RahmahNo ratings yet
- Transient Ischemic AttackDocument23 pagesTransient Ischemic AttackAnonymous 9xHTwHYNo ratings yet
- Acute Coronary Syndrome (ACS) : Basic Principles For ACSDocument4 pagesAcute Coronary Syndrome (ACS) : Basic Principles For ACSRendra DananjayaNo ratings yet
- Management of StrokeDocument24 pagesManagement of StrokeEngel TuranganNo ratings yet
- Acs 11 190524110746Document46 pagesAcs 11 190524110746Obakeng MandaNo ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Stroke Transient Ischaemic AttackDocument15 pagesStroke Transient Ischaemic AttackAarif RanaNo ratings yet
- Guidelines & Protocols: Stroke and Transient Ischemic Attack - Management and Prevention Advisory CommitteeDocument13 pagesGuidelines & Protocols: Stroke and Transient Ischemic Attack - Management and Prevention Advisory CommitteeAndi SaputraNo ratings yet
- Journal Reading Clopi Aspirin FinalDocument49 pagesJournal Reading Clopi Aspirin FinalWenny AnggonoNo ratings yet
- Hypertension I: by Ph. Sarah T. OmranDocument34 pagesHypertension I: by Ph. Sarah T. OmranMoataz MansourNo ratings yet
- DynaMed Plus - Stroke (Acute Management)Document126 pagesDynaMed Plus - Stroke (Acute Management)Sarah Shafa MarwadhaniNo ratings yet
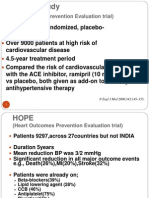
- The HOPE Study: (Heart Outcomes Prevention Evaluation Trial)Document4 pagesThe HOPE Study: (Heart Outcomes Prevention Evaluation Trial)kurutalaNo ratings yet
- After A Stroke or TIA - New Guidelines To Prevent Recurrence 2Document5 pagesAfter A Stroke or TIA - New Guidelines To Prevent Recurrence 2Javiera Paz Guerrero CassanelloNo ratings yet
- CHADS2 Score: For Other Uses, SeeDocument5 pagesCHADS2 Score: For Other Uses, SeeLiseth Victorio HuamanNo ratings yet
- Af IndigoDocument60 pagesAf IndigoLalrin ChhanaNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- Atherosclerotic Cardiovascular Disease (ASCVD) Secondary Prevention GuidelineDocument19 pagesAtherosclerotic Cardiovascular Disease (ASCVD) Secondary Prevention GuidelinearieftomNo ratings yet
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyDocument37 pagesPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaNo ratings yet
- Dyslipidaemias 2019Document30 pagesDyslipidaemias 2019Adinda DianNo ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Manajemen Hypertension in StrokeDocument14 pagesManajemen Hypertension in StrokeAdelaide SharfinaNo ratings yet
- Merec Bulletin Vol15 No6Document4 pagesMerec Bulletin Vol15 No6n4dn4dNo ratings yet
- Dual Antiplatelet Therapy After PCI in Patients atDocument32 pagesDual Antiplatelet Therapy After PCI in Patients atyamonaelgamNo ratings yet
- Ischemic Heart Diease PDFDocument33 pagesIschemic Heart Diease PDFMahamed Wefkey OmranNo ratings yet
- Early Antithrombotic Treatment of Acute Ischemic Stroke and Transient Ischemic Attack - UpToDateDocument27 pagesEarly Antithrombotic Treatment of Acute Ischemic Stroke and Transient Ischemic Attack - UpToDateEduardo QuinteroNo ratings yet
- Management of CADDocument99 pagesManagement of CADUmesh BabuNo ratings yet
- CCU HandoverDocument9 pagesCCU Handoverapi-192342497No ratings yet
- Outpatient MedicineDocument190 pagesOutpatient MedicineLikoh TimothyNo ratings yet
- Drugs ACSDocument5 pagesDrugs ACSGilbert NeahNo ratings yet
- A Broad Review of Hypertension Pharmacology: Eview RticleDocument5 pagesA Broad Review of Hypertension Pharmacology: Eview RticleAdeline KosmetikNo ratings yet
- NTGDocument47 pagesNTGAjeng TitiNo ratings yet
- Management of Acute Ischemic Stroke (AIS) DR GaneshDocument69 pagesManagement of Acute Ischemic Stroke (AIS) DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Dyslipidemia ATP4 GUIDLINESDocument9 pagesDyslipidemia ATP4 GUIDLINESSandy GunawanNo ratings yet
- Clopidogrel Plus Aspirin Vs Aspirin Alone For Acute Minor Ischaemic Stroke or High Risk TIA: Systematic Review and Meta-AnalysisDocument25 pagesClopidogrel Plus Aspirin Vs Aspirin Alone For Acute Minor Ischaemic Stroke or High Risk TIA: Systematic Review and Meta-AnalysisMaryam RehmanNo ratings yet
- Volatile Anaesthetic Myocardial Protection: A Review of The Current LiteratureDocument5 pagesVolatile Anaesthetic Myocardial Protection: A Review of The Current Literatureserena7205No ratings yet
- Navi Mumbai HospitalDocument8 pagesNavi Mumbai Hospital8108295484No ratings yet
- Yeast As A Tool in Cancer Research 2007Document441 pagesYeast As A Tool in Cancer Research 2007Doorsea100% (1)
- Poor and Rich CountriesDocument5 pagesPoor and Rich Countriestwentyeight28No ratings yet
- DrShakil - Specialist Family Medicin7Document5 pagesDrShakil - Specialist Family Medicin7AsadMahmoodNo ratings yet
- The Emergency ServicesDocument14 pagesThe Emergency ServicesFUMC ANTIPOLO ER DEPTNo ratings yet
- Estrella, Christian R.: Education: Far Eastern University, 2010Document3 pagesEstrella, Christian R.: Education: Far Eastern University, 2010Christian EstrellaNo ratings yet
- Control Questions AnsweredDocument6 pagesControl Questions AnsweredIzabella MonteiroNo ratings yet
- BillsDocument5 pagesBillsనీలం మధు సూధన్ రెడ్డిNo ratings yet
- History of Air Ambulance and MedevacDocument4 pagesHistory of Air Ambulance and Medevacapi-267200582No ratings yet
- ICAI HS360 WithoutDuductibleDocument52 pagesICAI HS360 WithoutDuductiblepadiNo ratings yet
- Official Resume ApplebachDocument3 pagesOfficial Resume Applebachapi-283260051No ratings yet
- Final Hospital Pharmacy Module 2Document6 pagesFinal Hospital Pharmacy Module 2Meryl Ann Ibarra-InganNo ratings yet
- MBA Report - IntellicareDocument11 pagesMBA Report - IntellicareKat Dela CruzNo ratings yet
- Open EMRDocument38 pagesOpen EMRSuhail BhatiaNo ratings yet
- Satff Nurse E-ToolDocument4 pagesSatff Nurse E-ToolCharissa Magistrado De LeonNo ratings yet
- Watchers' Class On Range of Motion (ROM) ExercisesDocument19 pagesWatchers' Class On Range of Motion (ROM) ExercisesMaumau Camba ZafraNo ratings yet
- Patton FullerDocument5 pagesPatton FullerJacques OwokelNo ratings yet
- Consecutive Sampling. Instrumen Yang Digunakan Untuk Variabel Independent IalahDocument14 pagesConsecutive Sampling. Instrumen Yang Digunakan Untuk Variabel Independent IalahHANA TRI AYU GASPARNo ratings yet
- Noun 2Document20 pagesNoun 2Rt SaragihNo ratings yet
- Night of The Living DeadDocument130 pagesNight of The Living DeadVeronica HansonNo ratings yet
- Active and Passive Voice ExerciseDocument2 pagesActive and Passive Voice Exerciseela garcia100% (1)
- Bahan Ajajar English II KeperawatanDocument49 pagesBahan Ajajar English II KeperawatanEchingt TukaNo ratings yet
- Portfolio ResumeDocument2 pagesPortfolio Resumeapi-437947672No ratings yet
- MP 13212Document15 pagesMP 13212Mauro Rojas ZúñigaNo ratings yet
- PanelDocument13 pagesPanelSaddam HussainNo ratings yet
- Reported SpeechDocument3 pagesReported SpeechReka KutasiNo ratings yet
- Nursing Record and ReportsDocument32 pagesNursing Record and ReportsOm VaishNav100% (1)