You might also like
- Endocrine DisordersDocument77 pagesEndocrine Disordersahmad100% (2)
- Child With Blood DisorderDocument126 pagesChild With Blood DisorderSivabarathy100% (1)
- Types of AnemiaDocument9 pagesTypes of AnemiaShine Reyes MackieNo ratings yet
- WelcomeDocument103 pagesWelcomeLyka BernalNo ratings yet
- Anemia: Presented byDocument36 pagesAnemia: Presented byParmvir Singh100% (1)
- Acute Cardiac AlterationsDocument38 pagesAcute Cardiac AlterationsJoyce SiosonNo ratings yet
- HYDROCEPHALUSDocument63 pagesHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Acid-Base Balance PDFDocument3 pagesAcid-Base Balance PDFjanet roosevelt100% (2)
- Acid-Base Balance PDFDocument10 pagesAcid-Base Balance PDFinah krizia lague100% (1)
- Management of Patient With AnemiaDocument58 pagesManagement of Patient With AnemiaDoaa HussainNo ratings yet
- Dyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingDocument19 pagesDyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingNaseem Bin YoosafNo ratings yet
- Coagulation DisordersDocument14 pagesCoagulation Disorderssusan_grace123No ratings yet
- Nephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)Document26 pagesNephrotic Syndrome: Prepared by Dr. Kawsar Ahmed Intern Dr. (TMMCH)GENERAL sharpNo ratings yet
- Umbilical Artery CatheterizationDocument11 pagesUmbilical Artery CatheterizationRhaq Sheldon-CoelhoNo ratings yet
- Renal Failure in ChildrenDocument43 pagesRenal Failure in Childrendennyyy175No ratings yet
- Fluids and Electrolytes-2Document82 pagesFluids and Electrolytes-2Jem Loterte100% (1)
- New Fluid and Electrolytes Therapy Toyinoriginali2againDocument55 pagesNew Fluid and Electrolytes Therapy Toyinoriginali2againt.baby100% (1)
- NCM 102 Pedia Nervous, Hema,,Renal, SkeletalDocument178 pagesNCM 102 Pedia Nervous, Hema,,Renal, SkeletalMika SamsonNo ratings yet
- RicketsDocument5 pagesRicketsNader SmadiNo ratings yet
- ErythropoisisDocument47 pagesErythropoisisDisha SuvarnaNo ratings yet
- EndocrineDocument12 pagesEndocrineAna FelNo ratings yet
- Fluid and Electrolytes Lecture NotesDocument85 pagesFluid and Electrolytes Lecture NotesVince Peliño De MesaNo ratings yet
- Maternity Nursing 2Document133 pagesMaternity Nursing 2Rick100% (1)
- Abnormalities of PuerperiumDocument70 pagesAbnormalities of PuerperiumYasmin SharmaNo ratings yet
- Pediatric G.I Disorders FinalDocument53 pagesPediatric G.I Disorders FinalRashid Hussain0% (1)
- Anaemia in Pregnancy: By-Dr. Soumya.p (2nd Yr PG) Mod - Dr. Rita. D (Professor and Hod)Document98 pagesAnaemia in Pregnancy: By-Dr. Soumya.p (2nd Yr PG) Mod - Dr. Rita. D (Professor and Hod)SoumyaNo ratings yet
- Endocrine Disorders TableDocument6 pagesEndocrine Disorders TablebarbaraNo ratings yet
- Fluid, Electrolyte, and Acid-Base BalanceDocument42 pagesFluid, Electrolyte, and Acid-Base BalanceRichelene Mae CanjaNo ratings yet
- Vital Signs: Aurora Roslin Samosa, Man RNDocument57 pagesVital Signs: Aurora Roslin Samosa, Man RNAlexander DontonNo ratings yet
- Medical Surgical NursingDocument66 pagesMedical Surgical Nursing04eden100% (3)
- Congenital Anomalies of KidneDocument7 pagesCongenital Anomalies of KidneSanthosh.S.U100% (2)
- Nephrotic and Nephritic SyndromesDocument27 pagesNephrotic and Nephritic SyndromesJoshua Smith100% (1)
- 5 Bleeding Disorders PPT EditedDocument87 pages5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNo ratings yet
- MenstruationDocument37 pagesMenstruationJoy JarinNo ratings yet
- Fluids Electrolytes - Acid-Base BalanceDocument11 pagesFluids Electrolytes - Acid-Base BalanceJhosita Flora Laroco100% (1)
- Empyema 171013100219Document23 pagesEmpyema 171013100219Mahmoud Abdel MoneimNo ratings yet
- Principles of Fluid Therapy On The Basis ofDocument29 pagesPrinciples of Fluid Therapy On The Basis ofhendrytzNo ratings yet
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)
- Fluids & Electrolyte NewDocument154 pagesFluids & Electrolyte NewMaria Visitacion100% (2)
- Thalassemia PDFDocument88 pagesThalassemia PDFshabrinaerin100% (1)
- IV FluidsDocument47 pagesIV FluidsMuvenn Kannan100% (1)
- Body Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionDocument33 pagesBody Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionMan LingNo ratings yet
- Disorders of The Genitourinary SystemDocument49 pagesDisorders of The Genitourinary SystemYemaya84No ratings yet
- Diagnostic TestingDocument10 pagesDiagnostic TestingVrindha Vijayan100% (1)
- Increased Intracranial PressureDocument34 pagesIncreased Intracranial PressureshykitijaNo ratings yet
- Neurologic System: Carolyn Jarvis Physical Examination and Health Assessment Fourth EditionDocument37 pagesNeurologic System: Carolyn Jarvis Physical Examination and Health Assessment Fourth Edition03152788100% (1)
- Eyes and Ears DisordersDocument36 pagesEyes and Ears Disordersjeshema100% (4)
- Neurological SystemDocument10 pagesNeurological SystemManelle SingzonNo ratings yet
- Enzymes of Clinical SignificanceDocument65 pagesEnzymes of Clinical SignificancepaulaOrialNo ratings yet
- Q. List Different Functions of The Kidney: (A) Homeostatic FunctionDocument42 pagesQ. List Different Functions of The Kidney: (A) Homeostatic Functionramadan100% (4)
- Respiratory System DisordersDocument353 pagesRespiratory System Disordersይደግ አብነውNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathySuhas KandeNo ratings yet
- Nursing Management in Abdominal SurgeryDocument19 pagesNursing Management in Abdominal Surgeryejguy7777100% (2)
- Anomalies of Skeletal System-1Document44 pagesAnomalies of Skeletal System-1Meena Koushal100% (1)
- Hemorrhagic Disease of The NewbornDocument2 pagesHemorrhagic Disease of The NewbornsucirahmiiiiiiNo ratings yet
- Leukemia in Children: 1 Rahul Dhaker, Asst. Professor, RCNDocument41 pagesLeukemia in Children: 1 Rahul Dhaker, Asst. Professor, RCNRahul DhakerNo ratings yet
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Acute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Infant Jaundice, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInfant Jaundice, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Critical ThinkingDocument6 pagesCritical ThinkingmatrixtrinityNo ratings yet
- Intelligence in PsychologyDocument29 pagesIntelligence in PsychologymatrixtrinityNo ratings yet
- Stress and Illness: Castillo, Justine GDocument19 pagesStress and Illness: Castillo, Justine GmatrixtrinityNo ratings yet
- Group Number: Case Title: Year and Section: Group Members: 1. 5. 2. 6. 3. 7. 4. 8Document1 pageGroup Number: Case Title: Year and Section: Group Members: 1. 5. 2. 6. 3. 7. 4. 8matrixtrinityNo ratings yet
- antepartumTEST1 MOSBYDocument14 pagesantepartumTEST1 MOSBYmatrixtrinity50% (2)
- Antepartumtest2 LippincottDocument7 pagesAntepartumtest2 Lippincottmatrixtrinity100% (1)
- Distinguishing Features of Anthropology - Characteristics 1-5 6.78 What Are The3 Unique Approaches of AnthropologyDocument2 pagesDistinguishing Features of Anthropology - Characteristics 1-5 6.78 What Are The3 Unique Approaches of AnthropologymatrixtrinityNo ratings yet
- Intestinal Obstruction5Document4 pagesIntestinal Obstruction5matrixtrinityNo ratings yet
- Socio - GENDER, ETHNICITY AND RACEDocument22 pagesSocio - GENDER, ETHNICITY AND RACEmatrixtrinity100% (1)
- Cardio DiseasesDocument17 pagesCardio DiseasesmatrixtrinityNo ratings yet
- Intestinal Obstruction Wit Pic2Document2 pagesIntestinal Obstruction Wit Pic2matrixtrinityNo ratings yet
- Blood ComponentDocument33 pagesBlood Componentmatrixtrinity100% (1)
- Cardiovascular Physio Logic ProcessDocument35 pagesCardiovascular Physio Logic ProcessmatrixtrinityNo ratings yet
- What Is Intestinal ObstructionDocument5 pagesWhat Is Intestinal ObstructionmatrixtrinityNo ratings yet
- Cerebrovascular Accidents: Rochee P. Benito, RNDocument23 pagesCerebrovascular Accidents: Rochee P. Benito, RNmatrixtrinityNo ratings yet
- Circulatory System: Rochi Paraon Benito, RN Infection Control NurseDocument15 pagesCirculatory System: Rochi Paraon Benito, RN Infection Control NursematrixtrinityNo ratings yet
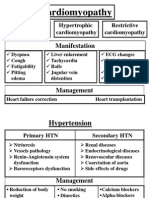
- Cardiomyopathy 02Document2 pagesCardiomyopathy 02matrixtrinityNo ratings yet
- Cardiovascular Therapeutic ManagementDocument15 pagesCardiovascular Therapeutic ManagementmatrixtrinityNo ratings yet
- Burns and Environmental EmergenciesDocument33 pagesBurns and Environmental EmergenciesmatrixtrinityNo ratings yet
- Nutritional Requirements in Pregnancy and LactationDocument12 pagesNutritional Requirements in Pregnancy and LactationPatrick nyawiraNo ratings yet
- Pharm MCQ BookDocument11 pagesPharm MCQ BookanojanNo ratings yet
- Therapeutic Interchange ListDocument29 pagesTherapeutic Interchange ListНазарій ЛавровськийNo ratings yet
- Anaemia in Pregnancy-MaklapDocument34 pagesAnaemia in Pregnancy-MaklapBronson KaturkanaNo ratings yet
- Parenteral Iron TherapyDocument31 pagesParenteral Iron TherapyEmmanuel Kissiedu Antiri100% (1)
- Lecture 29-AnemiaDocument35 pagesLecture 29-AnemiaBini JaminNo ratings yet
- CKD My PharmacotherapyDocument7 pagesCKD My PharmacotherapyJA TongNo ratings yet
- Oral Iron ProductsDocument2 pagesOral Iron ProductsOlga BabiiNo ratings yet
- An Approach To Anemic PatientDocument79 pagesAn Approach To Anemic PatientHussain AzharNo ratings yet
- OB Hematologic DiseasesDocument2 pagesOB Hematologic DiseasespreciousjemNo ratings yet
- Spectrophotometric Method For Quantitative Determination of Iron III From Iron Polymaltose ComplexDocument6 pagesSpectrophotometric Method For Quantitative Determination of Iron III From Iron Polymaltose ComplexAde MuchlasNo ratings yet
- Iron Nutrition and Lead ToxicityDocument32 pagesIron Nutrition and Lead ToxicityChibueze EzeokaforNo ratings yet
- Drug Study Ferrous SulfateDocument2 pagesDrug Study Ferrous SulfatePauline AnesNo ratings yet
- LP 1 I NCM 107 RLE I CARE OF PREGNANT WOMAN StudentsDocument28 pagesLP 1 I NCM 107 RLE I CARE OF PREGNANT WOMAN StudentsNaomi Anne AsuntoNo ratings yet
- Obs-UM - Paper - 1Document16 pagesObs-UM - Paper - 1Muhammad Abbas AliNo ratings yet
- Iron SucroseDocument3 pagesIron SucroseAtul KumarNo ratings yet
- Ferrous Sulfate Syrup InsertDocument6 pagesFerrous Sulfate Syrup InsertPrincess TiongsonNo ratings yet
- Tratamiento de Anemia Por Deficiencia de Hierro en Ancianos Nuevos ParadigmasDocument11 pagesTratamiento de Anemia Por Deficiencia de Hierro en Ancianos Nuevos ParadigmasCarlos OlivoNo ratings yet
- Agen HematinikDocument77 pagesAgen HematinikErinaGeraldiNo ratings yet
- What Causes Iron-Deficiency Anemia?Document54 pagesWhat Causes Iron-Deficiency Anemia?Zaia Raymond FlumoNo ratings yet
- Iron Dextran Drug StudyDocument5 pagesIron Dextran Drug StudySofronio OmboyNo ratings yet
- COMPILATIONSSSSDocument976 pagesCOMPILATIONSSSSANNooonynmousNo ratings yet
- Physiological C-WPS OfficeDocument15 pagesPhysiological C-WPS OfficeGwagsiGlennNo ratings yet
- Liposomal IronDocument6 pagesLiposomal IronPiyush KhetrapalNo ratings yet
- Deficiency Iron AnemiaDocument9 pagesDeficiency Iron AnemiaNadia Puspita DewiNo ratings yet
- AGA Technical Review On GI Evaluation of Iron Deficiency AnemiaDocument10 pagesAGA Technical Review On GI Evaluation of Iron Deficiency AnemiaElena ChNo ratings yet
- Anemia During PregnancyDocument7 pagesAnemia During Pregnancydita fNo ratings yet
- 813-Article Text-1261-1-10-20180214Document5 pages813-Article Text-1261-1-10-20180214dwiky ramaNo ratings yet
- Vi. Drug Study: Source: 2011 Lippincott's Nursing Drug GuideDocument8 pagesVi. Drug Study: Source: 2011 Lippincott's Nursing Drug GuideDarNo ratings yet
- KU - Lesson 4A - DRUGS USED IN ANAEMIADocument60 pagesKU - Lesson 4A - DRUGS USED IN ANAEMIAchristine gisembaNo ratings yet