You might also like
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Internship ManualDocument10 pagesInternship ManualChloe JazminesNo ratings yet
- Pharmacy and Therapeutics Committee Policies and ProceduresDocument5 pagesPharmacy and Therapeutics Committee Policies and ProceduresPHARMACY OLMCMCNo ratings yet
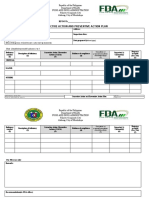
- Corrective Action and Preventive Action Plan: RFO/CODocument3 pagesCorrective Action and Preventive Action Plan: RFO/COAlfred John TrinidadNo ratings yet
- White and Red Label - PharmacyDocument3 pagesWhite and Red Label - Pharmacysheryl GuillermoNo ratings yet
- Therapeutics Committee ManualDocument49 pagesTherapeutics Committee Manualdarkhawk44100% (1)
- Philippines Sales and Promotion FDA OutlineDocument30 pagesPhilippines Sales and Promotion FDA OutlineAidee SmithNo ratings yet
- Generic Dispensing Flowchart: Over The Counter Drugs Prescription Drugs (RX)Document1 pageGeneric Dispensing Flowchart: Over The Counter Drugs Prescription Drugs (RX)chibibi the grNo ratings yet
- Joint Affidavit of UndertakingDocument1 pageJoint Affidavit of UndertakingMyzhel Inumerable100% (1)
- Generic Menu CardDocument9 pagesGeneric Menu CardLode DeocadesNo ratings yet
- FermentationDocument38 pagesFermentationlorraine_cuaNo ratings yet
- FermentationDocument38 pagesFermentationlorraine_cuaNo ratings yet
- Activity 11 19Document23 pagesActivity 11 19RyannDeLeonNo ratings yet
- Good Dispensing PracticeDocument59 pagesGood Dispensing Practicechalii100% (1)
- Generic Menu CardDocument7 pagesGeneric Menu CardDee BelarminoNo ratings yet
- Unit 1. Clinical PharmacyDocument5 pagesUnit 1. Clinical PharmacyAashish BhattaraiNo ratings yet
- Restricted Drugs and Non FormularyDocument2 pagesRestricted Drugs and Non FormularyChristine Joy De OcampoNo ratings yet
- For External Use Only For External Use OnlyDocument1 pageFor External Use Only For External Use OnlyRacel BandongNo ratings yet
- Ra 9711Document15 pagesRa 9711Johnny ManahanNo ratings yet
- Ra 10918 PDFDocument19 pagesRa 10918 PDFJohn Fritz Gerald BascoNo ratings yet
- Control of The Practice of Pharmacy.Document4 pagesControl of The Practice of Pharmacy.RANIELLE SIMNo ratings yet
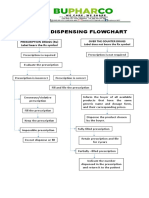
- Generic Dispensing FlowchartDocument1 pageGeneric Dispensing FlowchartBUPHARCO Mintal Branch100% (1)
- Sop RXDocument13 pagesSop RXGloria RamosNo ratings yet
- Patient Medication Profile and CounselingDocument56 pagesPatient Medication Profile and CounselingMeimei QueNo ratings yet
- Nurse Orientation - NarcoticsDocument25 pagesNurse Orientation - NarcoticsSalma MustafaNo ratings yet
- Shu ACT 2Document4 pagesShu ACT 2John Daniel CapituloNo ratings yet
- Handling and Monitoring of Dangerous DrugsDocument10 pagesHandling and Monitoring of Dangerous DrugsRadz BolambaoNo ratings yet
- Legal Pharm Course OutlineDocument69 pagesLegal Pharm Course OutlineLysa VeeNo ratings yet
- t11 Reaction Kinetics 19-26Document7 pagest11 Reaction Kinetics 19-26lorraine_cuaNo ratings yet
- DISPENSINGDocument26 pagesDISPENSINGash currieNo ratings yet
- Role and Responsibility of Pharmacy Assistant in Community PharmacyDocument4 pagesRole and Responsibility of Pharmacy Assistant in Community PharmacyUntouchable Monster 2No ratings yet
- M2 - Lesson 1 - Preparation of Standard Patient ScriptingDocument22 pagesM2 - Lesson 1 - Preparation of Standard Patient ScriptingElleason Joshua G. FranciscoNo ratings yet
- Duties and Responsibilities - Pharmacy BusinessDocument4 pagesDuties and Responsibilities - Pharmacy BusinessMA. TRIXIA ANNE KAHULUGANNo ratings yet
- RegistrationDocument130 pagesRegistrationJoanne AquinoNo ratings yet
- Government Mediated Access Price 2016Document3 pagesGovernment Mediated Access Price 2016JoshNo ratings yet
- Joint Dti-Da-Doe Adm Order No. 17-02 - s2017Document5 pagesJoint Dti-Da-Doe Adm Order No. 17-02 - s2017crazzy foryouNo ratings yet
- Republic Act. 5921 - Pharmacy LawDocument14 pagesRepublic Act. 5921 - Pharmacy LawSunshine_Bacla_4275100% (1)
- Module 2 Licensing of Drug Outlets and Pharmaceutical EstablishmentsDocument28 pagesModule 2 Licensing of Drug Outlets and Pharmaceutical EstablishmentsELLEN NAE MONTRIASNo ratings yet
- Joint Affidavit: Republic of The Philippines) ) S.SDocument1 pageJoint Affidavit: Republic of The Philippines) ) S.SEdgar Soller JrNo ratings yet
- Drug Approval System of The Philippines PDFDocument56 pagesDrug Approval System of The Philippines PDFPatrick OribelloNo ratings yet
- Cpi - Damasco - Activity 25 & 26Document3 pagesCpi - Damasco - Activity 25 & 26LDCU - Damasco, Erge Iris M.No ratings yet
- Seatwork 2Document1 pageSeatwork 2Kenny TuanNo ratings yet
- Nica Chua-JournalDocument7 pagesNica Chua-JournalMa Victoria ChuaNo ratings yet
- Biosimilars Advantages and DisadvantagesDocument2 pagesBiosimilars Advantages and DisadvantagesVeeda CR100% (1)
- Internship5 12Document7 pagesInternship5 12Jerel MarquezNo ratings yet
- Doh Ao 2017Document11 pagesDoh Ao 2017graceNo ratings yet
- MSPH 600 Ao 64 S. 1989 ReportDocument6 pagesMSPH 600 Ao 64 S. 1989 ReportShynne RPhNo ratings yet
- Exercises 8-10 (By Dr. N. Tubon) PDFDocument25 pagesExercises 8-10 (By Dr. N. Tubon) PDFLoren100% (1)
- Ali Medicos Pharmacy Standard Operating Procedures (Sops)Document4 pagesAli Medicos Pharmacy Standard Operating Procedures (Sops)Amir ZakiNo ratings yet
- Pharmacist Licensure ExamDocument2 pagesPharmacist Licensure ExamIna GuinarNo ratings yet
- Cpi - Activity No. 9Document4 pagesCpi - Activity No. 9Aila Marie ArandillaNo ratings yet
- Railway PharmasistDocument2 pagesRailway PharmasistprashantNo ratings yet
- Government Mediated Access Price PhilippinesDocument4 pagesGovernment Mediated Access Price PhilippinesKristin0% (2)
- Dispensing ChecklistDocument2 pagesDispensing Checklistsafia321No ratings yet
- Ra 9502Document22 pagesRa 9502Are Pee EtcNo ratings yet
- Patient Database Form, DTPW, PCPDocument7 pagesPatient Database Form, DTPW, PCPClarence100% (1)
- BFADDocument4 pagesBFADKc Ganda BNo ratings yet
- Manual - PrescriptionDocument5 pagesManual - PrescriptionRyan Glenn SoguilonNo ratings yet
- Hospital Pharmacy ProfileDocument7 pagesHospital Pharmacy ProfileJessica BautistaNo ratings yet
- REQUIREMENTS FOR Bfad Medical Device DistrutorDocument3 pagesREQUIREMENTS FOR Bfad Medical Device DistrutorEvanz Denielle A. OrbonNo ratings yet
- Annex CDDocument3 pagesAnnex CDAllen MedinaNo ratings yet
- Petition FormDocument1 pagePetition FormAmaeten100% (1)
- Petition Form HHS 2013 FINALDocument1 pagePetition Form HHS 2013 FINALTimothy Robert MutiaNo ratings yet
- Chap 13 Mod 1Document70 pagesChap 13 Mod 1lorraine_cuaNo ratings yet
- ' Heat StrokeDocument7 pages' Heat Strokelorraine_cuaNo ratings yet
- Chemistry 132 NT: Nothing Great Was Ever Achieved Without EnthusiasmDocument50 pagesChemistry 132 NT: Nothing Great Was Ever Achieved Without Enthusiasmlorraine_cuaNo ratings yet
- Chapt29 ImageDocument53 pagesChapt29 Imagelorraine_cuaNo ratings yet
- VaccineDocument1 pageVaccinelorraine_cuaNo ratings yet
- DominicDocument6 pagesDominiclorraine_cuaNo ratings yet
- Tro 13 KineticsDocument13 pagesTro 13 KineticsNikoletta StrandbergNo ratings yet
- Reaction Mech For Ether and EpoxidDocument59 pagesReaction Mech For Ether and Epoxidlorraine_cuaNo ratings yet
- Effects of Ginger On The Improvement of Asthma (The Evaluation of Its' Treatmental Effects)Document4 pagesEffects of Ginger On The Improvement of Asthma (The Evaluation of Its' Treatmental Effects)lorraine_cuaNo ratings yet
- Organic Polymer ChemistryDocument23 pagesOrganic Polymer Chemistrylorraine_cua100% (1)
- Cation SDocument56 pagesCation Slorraine_cua100% (1)
- Oppositional InferenceDocument4 pagesOppositional Inferencelorraine_cuaNo ratings yet