You might also like
- New Patient Application UpdatedDocument5 pagesNew Patient Application UpdatedAbdu AryaNo ratings yet
- Assessment Sheet Rev 2Document2 pagesAssessment Sheet Rev 2meghanNo ratings yet
- FCA QuestionnaireDocument8 pagesFCA QuestionnaireAevah QuinnNo ratings yet
- Medical History FormDocument2 pagesMedical History Formapi-279870303No ratings yet
- Unit 829 Level 3 Provide Spa Treatments Treatment Evidence FormDocument4 pagesUnit 829 Level 3 Provide Spa Treatments Treatment Evidence FormJowie SooNo ratings yet
- Consultation From For SpaDocument2 pagesConsultation From For Spafpmwjh5n9vNo ratings yet
- History TakingDocument2 pagesHistory TakingAmbar Rashid100% (1)
- History Taking ChecklistDocument4 pagesHistory Taking Checklistalnoooor38100% (1)
- Personal Trainer Consultation FormDocument3 pagesPersonal Trainer Consultation Formsamssgrr1100% (4)
- New Patient History FormDocument6 pagesNew Patient History Formعبدالله الكافNo ratings yet
- Case Record PDFDocument31 pagesCase Record PDFAmey JatharNo ratings yet
- Medical History Record: For Faster Service, Please Complete The Following Form Prior To Arriving at Our OfficeDocument1 pageMedical History Record: For Faster Service, Please Complete The Following Form Prior To Arriving at Our OfficeRichard SazoNo ratings yet
- Your Health PlanDocument9 pagesYour Health PlanMaggie FornaroNo ratings yet
- Medical Questionnaire Forms-2Document1 pageMedical Questionnaire Forms-2chemkumar16No ratings yet
- Massage Client Intake Form: Personal InformationDocument1 pageMassage Client Intake Form: Personal InformationTreicy AguileraNo ratings yet
- Golden+Yogi+Health+Assessment+Form Doc-2Document9 pagesGolden+Yogi+Health+Assessment+Form Doc-2ohasfwaNo ratings yet
- Medical History FormDocument1 pageMedical History Form2oclockNo ratings yet
- Electronic Health Record (EHR) of Click Health Services Care Receiver (CR)Document10 pagesElectronic Health Record (EHR) of Click Health Services Care Receiver (CR)Himel Baidya HimuNo ratings yet
- Electronic Health Record (EHR) of Click Health Services Care Receiver (CR)Document10 pagesElectronic Health Record (EHR) of Click Health Services Care Receiver (CR)Himel Baidya HimuNo ratings yet
- Case Record Book EnglishDocument31 pagesCase Record Book EnglishBabli Lovely Nicky100% (1)
- Patient History FormDocument3 pagesPatient History FormFazal MehmoodNo ratings yet
- Patient Health Assessment PDFDocument8 pagesPatient Health Assessment PDFVictor BarbosaNo ratings yet
- PPGMedical History FormDocument2 pagesPPGMedical History Formmb344617No ratings yet
- History Taking FormDocument9 pagesHistory Taking FormEren ErkılınçNo ratings yet
- Adult Medical History Form: Please Complete All Pages NameDocument5 pagesAdult Medical History Form: Please Complete All Pages NameCaroline IberfuentesNo ratings yet
- Oriental Medicine Patient Intake FormDocument1 pageOriental Medicine Patient Intake FormMary AndersonNo ratings yet
- Student Health Form: General InformationDocument1 pageStudent Health Form: General Informationreza329329No ratings yet
- (Internal Use Only) (Internal Use Only) : (Cola, Coffee, Tea, or Chocolate)Document3 pages(Internal Use Only) (Internal Use Only) : (Cola, Coffee, Tea, or Chocolate)peachycreampup1763No ratings yet
- NP Intake FormDocument6 pagesNP Intake FormaweaverdcNo ratings yet
- Orthopedics Nerve InjuryDocument6 pagesOrthopedics Nerve InjuryPravinNo ratings yet
- Goroll - Primary Care Medicine Recommendations 1st EdDocument413 pagesGoroll - Primary Care Medicine Recommendations 1st EdalessandrocorreadasilvaNo ratings yet
- Pemeriksaaan Fisik AnakDocument124 pagesPemeriksaaan Fisik AnakNicole Ngo100% (1)
- OB-GYN Intake Form New Patient InformationDocument6 pagesOB-GYN Intake Form New Patient InformationaltenereNo ratings yet
- Family First Chiropractic Client Intake 03172Document6 pagesFamily First Chiropractic Client Intake 03172Trina AsterinoNo ratings yet
- Case Record PDFDocument31 pagesCase Record PDFShakti RakholiyaNo ratings yet
- Homeopathy Questionnaire 2Document30 pagesHomeopathy Questionnaire 2SanjeevNo ratings yet
- Fit To Work Certificate DocxDocument3 pagesFit To Work Certificate DocxBlood ViernesNo ratings yet
- History Taking Orthopaedics CompleteDocument6 pagesHistory Taking Orthopaedics CompletenorisahnirishNo ratings yet
- COMPLETE HISTORY WRITE UP 10.19 NewDocument3 pagesCOMPLETE HISTORY WRITE UP 10.19 NewAji PicanteNo ratings yet
- CaseperformaDocument7 pagesCaseperformaSandip VaghelaNo ratings yet
- Medical History Form Patient Medical History: (Specify)Document2 pagesMedical History Form Patient Medical History: (Specify)ian mNo ratings yet
- BokSmart - General Medical AssessmentDocument12 pagesBokSmart - General Medical AssessmentDirko SmutsNo ratings yet
- Ulcer Performas 01Document5 pagesUlcer Performas 01atharva sawantNo ratings yet
- Case Record FormDocument30 pagesCase Record FormVirag Patil100% (1)
- Orthopaedic Patient History Name: Date: AgeDocument3 pagesOrthopaedic Patient History Name: Date: AgeBedahulm XNo ratings yet
- History TakingDocument55 pagesHistory TakingDeepika MahajanNo ratings yet
- Med Q English PDFDocument2 pagesMed Q English PDFxryanxNo ratings yet
- Orthopaedic History FormDocument3 pagesOrthopaedic History FormtamikanjiNo ratings yet
- Homeopathy Case TakingDocument19 pagesHomeopathy Case Takingjasoneinstein100% (1)
- 2 Adult Case FormDocument28 pages2 Adult Case Formmahdeforouzesh.publicationNo ratings yet
- Newpatient FormsDocument2 pagesNewpatient Formsapi-239262305No ratings yet
- OSCE NotesDocument4 pagesOSCE NotesHighschool AudiobooksNo ratings yet
- LLC Health FormDocument2 pagesLLC Health Formcesar maguigadNo ratings yet
- Medicine General HXDocument5 pagesMedicine General HXudazxfNo ratings yet
- Health History AdultDocument5 pagesHealth History AdultchocobuniNo ratings yet
- Health Declaration Form14 - 2022Document3 pagesHealth Declaration Form14 - 2022DawnNo ratings yet
- Acupuncture Patient Intake FormDocument4 pagesAcupuncture Patient Intake FormRomans 6:23100% (1)
- Pre Employment Medical TestDocument2 pagesPre Employment Medical TestRamanan BothuNo ratings yet
- Blog-eBooks The Smart Way Pat FlynnDocument35 pagesBlog-eBooks The Smart Way Pat Flynnjbiddy789No ratings yet
- Normal Lab References For NCLEXDocument3 pagesNormal Lab References For NCLEXtotodile23No ratings yet
- Fluid & Electrolytes Study GuideDocument3 pagesFluid & Electrolytes Study GuideTofan AnaNo ratings yet
- Beachbody Insanity Custom Chart - Version 1.0 PDFDocument1 pageBeachbody Insanity Custom Chart - Version 1.0 PDFDavid BerissoNo ratings yet
- N361 Fluid and Electrolytes TableDocument14 pagesN361 Fluid and Electrolytes TableTofan AnaNo ratings yet
- Normal Lab References For NCLEXDocument3 pagesNormal Lab References For NCLEXtotodile23No ratings yet
- Study Guide For Fluid and ElectrolytesDocument4 pagesStudy Guide For Fluid and ElectrolytesTofan AnaNo ratings yet
- ES Price List 2014 With SkillsDocument2 pagesES Price List 2014 With SkillsTofan AnaNo ratings yet
- Electrolyte CompleteDocument6 pagesElectrolyte CompleteTofan Ana100% (2)
- Osteoblastic Tumors MSK Part IDocument51 pagesOsteoblastic Tumors MSK Part ITofan AnaNo ratings yet
- ETHICON Encyclopedia of Knots (Noduri Chirurgicale PDFDocument49 pagesETHICON Encyclopedia of Knots (Noduri Chirurgicale PDFoctav88No ratings yet
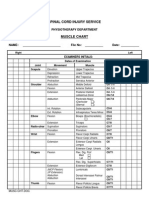
- Misc Physiotherapy Department Muscle Chart 2011Document2 pagesMisc Physiotherapy Department Muscle Chart 2011Tofan AnaNo ratings yet
- Directia Relatii Internationale International Relations DepartmentDocument2 pagesDirectia Relatii Internationale International Relations DepartmentTofan AnaNo ratings yet
- Use The Chart Below To Estimate Your Pain LevelDocument1 pageUse The Chart Below To Estimate Your Pain LevelTofan AnaNo ratings yet
- Measurement Model Tests Children Cerebral Palsy LessonsDocument16 pagesMeasurement Model Tests Children Cerebral Palsy LessonsTofan AnaNo ratings yet
- Get Shredded 2Document30 pagesGet Shredded 2Tofan AnaNo ratings yet
- Ghid or AutismDocument36 pagesGhid or Autismlaura_hajdu100% (3)
- StretchingDocument32 pagesStretchingTofan Ana88% (8)
- Act-Now Fact Sheet 35: Developing Gross Motor SkillsDocument5 pagesAct-Now Fact Sheet 35: Developing Gross Motor SkillsTofan AnaNo ratings yet