You might also like
- The Inner Cause: A Psychology of Symptoms from A to ZFrom EverandThe Inner Cause: A Psychology of Symptoms from A to ZRating: 5 out of 5 stars5/5 (2)
- History Taking FormDocument9 pagesHistory Taking FormEren ErkılınçNo ratings yet
- Medical History FormDocument2 pagesMedical History FormUtkarsh LakraNo ratings yet
- Patient Assessment Form For AdultsDocument2 pagesPatient Assessment Form For AdultsAriane CauanNo ratings yet
- Case Taking FormatDocument29 pagesCase Taking FormatmadhukarNo ratings yet
- Health History FormDocument9 pagesHealth History FormD2WNo ratings yet
- Adult Med HXDocument2 pagesAdult Med HXapi-3868874No ratings yet
- Patient Evaluation Form - Cerebral Palsy: Click or Use The TAB Key To Move Between FieldsDocument7 pagesPatient Evaluation Form - Cerebral Palsy: Click or Use The TAB Key To Move Between FieldsSyed Ali ShahNo ratings yet
- Patient Registration FormDocument5 pagesPatient Registration FormCari WithrowNo ratings yet
- HOMEOPATHIC CASE FORMATDocument21 pagesHOMEOPATHIC CASE FORMATSatyendra Rawat43% (7)
- Chemical Dependency EvaluationDocument1 pageChemical Dependency EvaluationBekki JonesNo ratings yet
- 2 Adult Case FormDocument28 pages2 Adult Case Formmahdeforouzesh.publicationNo ratings yet
- Homeopathy Questionnaire 2Document30 pagesHomeopathy Questionnaire 2SanjeevNo ratings yet
- Family First Chiropractic Client Intake 03172Document6 pagesFamily First Chiropractic Client Intake 03172Trina AsterinoNo ratings yet
- New Patient Health History FormDocument2 pagesNew Patient Health History FormKevinNo ratings yet
- PPGMedical History FormDocument2 pagesPPGMedical History Formmb344617No ratings yet
- Medical History QuestionnaireDocument1 pageMedical History QuestionnaireHare MasterYodaNo ratings yet
- Medical History FormDocument3 pagesMedical History FormSonja OsmanovićNo ratings yet
- Medical History FormDocument2 pagesMedical History Formapi-279870303No ratings yet
- Medical History Form Patient Medical History: (Specify)Document2 pagesMedical History Form Patient Medical History: (Specify)ian mNo ratings yet
- Patient Health Assessment PDFDocument8 pagesPatient Health Assessment PDFVictor BarbosaNo ratings yet
- Your Health HistoryDocument19 pagesYour Health Historyjasoneinstein100% (1)
- CWH OB-GYN History 011222Document2 pagesCWH OB-GYN History 011222alikhanomer5No ratings yet
- Golden+Yogi+Health+Assessment+Form Doc-2Document9 pagesGolden+Yogi+Health+Assessment+Form Doc-2ohasfwaNo ratings yet
- Rahaf Wardeh Internal Medicine 2016-2017Document4 pagesRahaf Wardeh Internal Medicine 2016-2017asdddNo ratings yet
- Fitness Assessment Questionnaire PDFDocument4 pagesFitness Assessment Questionnaire PDFKatrina Pillagara0% (1)
- PWDT (Pharmacist Workup Plan and TherapyDocument22 pagesPWDT (Pharmacist Workup Plan and TherapyAli HussnainNo ratings yet
- Volusia Obstetrics and GynecologyDocument2 pagesVolusia Obstetrics and Gynecologymee youNo ratings yet
- Cancer Health History FormDocument6 pagesCancer Health History FormShriNo ratings yet
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocument22 pagesPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordputihatauhitamNo ratings yet
- Health Declaration Form14 - 2022Document3 pagesHealth Declaration Form14 - 2022DawnNo ratings yet
- Case Record PDFDocument31 pagesCase Record PDFShakti RakholiyaNo ratings yet
- Patient History Form: 1 Physician InitialsDocument4 pagesPatient History Form: 1 Physician InitialsHenok TamiruNo ratings yet
- Patient History FormDocument4 pagesPatient History Formmirha fatima100% (1)
- Pt Medi History Form M2Document4 pagesPt Medi History Form M2Muhammad SyaifudinNo ratings yet
- Travel Questionnaire TemplateDocument6 pagesTravel Questionnaire TemplateNikhil JoharNo ratings yet
- Hypertension Follow Up EvaluationDocument1 pageHypertension Follow Up Evaluatione-MedTools100% (3)
- Northwest Medicine Travel Screening QuestionnaireDocument2 pagesNorthwest Medicine Travel Screening QuestionnaireMark Philipp AbanNo ratings yet
- Questionnaire EformDocument8 pagesQuestionnaire Eformrahul krishnanNo ratings yet
- PATIENT HISTORY FORMDocument4 pagesPATIENT HISTORY FORMEca SaputriNo ratings yet
- Case Record Book EnglishDocument31 pagesCase Record Book EnglishBabli Lovely Nicky100% (1)
- Health history questionnaireDocument3 pagesHealth history questionnaireVignesh VijayNo ratings yet
- 63925fbf4677a6ba79885506 - Medical History FormDocument3 pages63925fbf4677a6ba79885506 - Medical History FormAyunda PutriNo ratings yet
- Questioner: 1.personal InformationDocument2 pagesQuestioner: 1.personal InformationDr-Adnan Sarwar ChaudharyNo ratings yet
- (Neuro) Clinical Performa of 8th SemsDocument5 pages(Neuro) Clinical Performa of 8th SemsMuhammad Faizan RafiqNo ratings yet
- Ob History Form PDFDocument2 pagesOb History Form PDFRoan Marie JumaquioNo ratings yet
- dermato history formDocument1 pagedermato history formlaila.forestaNo ratings yet
- Psychiatry EvaluationDocument3 pagesPsychiatry Evaluatione-MedTools83% (24)
- New Patient Medical HistoryDocument3 pagesNew Patient Medical HistorybasheNo ratings yet
- History of cough, URTI, depression, dysuria, and dyslipidemia counselingDocument12 pagesHistory of cough, URTI, depression, dysuria, and dyslipidemia counselingSarah ANo ratings yet
- Northwestern Lifestyle Medicine QuestionnaireDocument9 pagesNorthwestern Lifestyle Medicine QuestionnaireAndrew HuaNo ratings yet
- Progresivve New FormDocument8 pagesProgresivve New FormZahir MalavéNo ratings yet
- Rheumatology Patient HistoryDocument5 pagesRheumatology Patient HistoryVidya VidyutNo ratings yet
- Case StudyDocument18 pagesCase StudyHanna Evidente BakalNo ratings yet
- Dokumen - Tips - TPN PWDT FormpdfDocument22 pagesDokumen - Tips - TPN PWDT FormpdfRao SohaibNo ratings yet
- Child Adol Traditional Biopsychosocial TemplateDocument11 pagesChild Adol Traditional Biopsychosocial Templateyeney armenteros100% (1)
- Up Form No2Document2 pagesUp Form No2Mitch Elle InfanteNo ratings yet
- Patient Registration FormDocument5 pagesPatient Registration FormAbdu AryaNo ratings yet
- Patient History Edited 2019Document3 pagesPatient History Edited 2019api-468186696No ratings yet
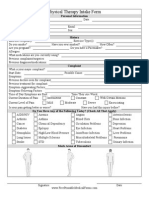
- Physical Therapy Intake FormDocument1 pagePhysical Therapy Intake FormTofan AnaNo ratings yet
- 21 - Piriformis SyndromeDocument11 pages21 - Piriformis SyndromewatiNo ratings yet
- November 2022 Philippine Nurse Licensure Examination ResultsDocument6 pagesNovember 2022 Philippine Nurse Licensure Examination ResultsRappler0% (1)
- The Tamil Nadu Dr. M.G.R. Medical University, CHENNAI - 600 032Document18 pagesThe Tamil Nadu Dr. M.G.R. Medical University, CHENNAI - 600 032ArtemisNo ratings yet
- Improve Balance and Coordination with Soccer LessonsDocument9 pagesImprove Balance and Coordination with Soccer LessonsAlvin Corpuz JrNo ratings yet
- Sociological Theories of Deviance: Definitions & ConsiderationsDocument10 pagesSociological Theories of Deviance: Definitions & ConsiderationsP TejeswariNo ratings yet
- The Nursing Process OverviewDocument26 pagesThe Nursing Process OverviewAYO NELSONNo ratings yet
- B.O. No. 1 S. 2023Document3 pagesB.O. No. 1 S. 2023edvince mickael bagunas sinonNo ratings yet
- Grade 8 BowDocument7 pagesGrade 8 BowJorely Barbero MundaNo ratings yet
- Ecological Systems Theory by Bronfenbrenner: Prepared By: Karen B. Reginaldo Jung PuertoDocument20 pagesEcological Systems Theory by Bronfenbrenner: Prepared By: Karen B. Reginaldo Jung Puertochristian ferrerNo ratings yet
- HTTPS: - Dacemirror - Sci-Hub - TW - Journal-Article - Soares2017 PDFDocument10 pagesHTTPS: - Dacemirror - Sci-Hub - TW - Journal-Article - Soares2017 PDFdarinsafinazNo ratings yet
- Conjoint Family Therapy - Book ReviewiewDocument4 pagesConjoint Family Therapy - Book Reviewiewkarunnal100% (2)
- Tutorial 1A - Public HealthDocument22 pagesTutorial 1A - Public Healthmuhammad saufi sulaimanNo ratings yet
- Psikososial Dan Budaya Dalam KeperawatanDocument11 pagesPsikososial Dan Budaya Dalam KeperawatanMohamad SyakiebNo ratings yet
- Nursing Care of The Older Adult in Wellness: Geriatric Nursing AssessmentDocument36 pagesNursing Care of The Older Adult in Wellness: Geriatric Nursing AssessmentRuby Corazon Ediza100% (6)
- Immediate Dentures ExplainedDocument64 pagesImmediate Dentures ExplainedDHANASRI MOTAPARTHYNo ratings yet
- Sample Af Form 860aDocument2 pagesSample Af Form 860aelsalenNo ratings yet
- ABP - MPDO Lakkireddy Palli Mandal Approved LetterDocument3 pagesABP - MPDO Lakkireddy Palli Mandal Approved Letterchild development project officer lakkireddypalliNo ratings yet
- Pool Paint Safety Data SheetDocument9 pagesPool Paint Safety Data SheetNicholson Vhenz UyNo ratings yet
- Dec 2 2022 Cot 1Document54 pagesDec 2 2022 Cot 1Estela AnchetaNo ratings yet
- Epidemiological StudiesDocument14 pagesEpidemiological StudiesMuhammad Touseef TahirNo ratings yet
- GMLOPS 2023 - 07 Company Rebranding Revised Panel Rates - Apr2023Document3 pagesGMLOPS 2023 - 07 Company Rebranding Revised Panel Rates - Apr2023KOONo ratings yet
- Professional Adjustment GuideDocument57 pagesProfessional Adjustment Guidemark OrpillaNo ratings yet
- Ethics in ResearchDocument29 pagesEthics in ResearchnationindiaNo ratings yet
- UPSC Prelims 2021 Geography Revision: High Probable Topics Part 2Document86 pagesUPSC Prelims 2021 Geography Revision: High Probable Topics Part 2PreethiNo ratings yet
- Board and Reviewer Assignments for Convened IRB ReviewDocument5 pagesBoard and Reviewer Assignments for Convened IRB ReviewMuhammad Zaryab KhanNo ratings yet
- List of Approved INGOsDocument4 pagesList of Approved INGOsZain JavedNo ratings yet
- Time Magazine USA - December 22 2023Document98 pagesTime Magazine USA - December 22 2023paccs2006No ratings yet
- B NursingDocument10 pagesB NursingAyeshia OliverNo ratings yet
- Indian EthosDocument19 pagesIndian Ethosshahid veettil100% (2)
- Removable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSDocument17 pagesRemovable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSAna MaríaNo ratings yet