You might also like
- Handbook of Nonprescription DrugsDocument5 pagesHandbook of Nonprescription DrugsHaris Abine Fatih0% (8)
- Se Insulin Stability ChartDocument2 pagesSe Insulin Stability ChartWirmanNo ratings yet
- Gastroenterology Evaluation TemplateDocument2 pagesGastroenterology Evaluation Templatee-MedTools86% (7)
- Complementary & Alternative MedicineDocument39 pagesComplementary & Alternative MedicineNengah TiastiningsihNo ratings yet
- MTHFR MutationDocument1 pageMTHFR MutationRobin KallisNo ratings yet
- FNE Anthropometrics Blood Pressure Companion Guide v8Document16 pagesFNE Anthropometrics Blood Pressure Companion Guide v8LeandroNunesAzevedo100% (1)
- Confidential Client Case History and Intake FormDocument1 pageConfidential Client Case History and Intake FormlunaNo ratings yet
- Low Copper Diet Plan & Shopping GuideDocument1 pageLow Copper Diet Plan & Shopping GuidePaulaNo ratings yet
- MTHFR Support Australia Sulphur Containing FoodsDocument2 pagesMTHFR Support Australia Sulphur Containing FoodsLisha HarbNo ratings yet
- Brightstone Transitions Medical HistoryDocument5 pagesBrightstone Transitions Medical HistoryRidhwan Hakim ZainurinNo ratings yet
- Abcds of Functional Nutrition Assessment-Nutrition Physical Exam & Lab RequestDocument7 pagesAbcds of Functional Nutrition Assessment-Nutrition Physical Exam & Lab Requestdocerick87No ratings yet
- Protocols@Internal Medicine@2018-2019Document54 pagesProtocols@Internal Medicine@2018-2019Sujeet ShahNo ratings yet
- Electrolyte and Metabolic Panel GuideDocument24 pagesElectrolyte and Metabolic Panel GuideDanish KamalNo ratings yet
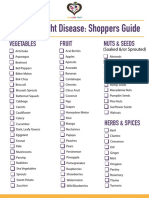
- Fight Disease Naturally with Foods from this Shoppers GuideDocument2 pagesFight Disease Naturally with Foods from this Shoppers GuidesrhhlyNo ratings yet
- Download Free Videos and PDF Articles on Inflammation and NutritionDocument31 pagesDownload Free Videos and PDF Articles on Inflammation and Nutritiontaoglider6902No ratings yet
- Medical Guide to Postural Tachycardia Syndrome (PoTSDocument12 pagesMedical Guide to Postural Tachycardia Syndrome (PoTSAttis PhrygiaNo ratings yet
- Health Pack For Oligospermia or Low sperm count शुक्राणु की कमी के लक्षण और दवा - NidanamDocument6 pagesHealth Pack For Oligospermia or Low sperm count शुक्राणु की कमी के लक्षण और दवा - NidanamsubratNo ratings yet
- Fat Restricted Diet (30 40 Grams) : PurposeDocument3 pagesFat Restricted Diet (30 40 Grams) : PurposeJonasDispersynNo ratings yet
- Testing Services Overview: Advanced Clinical Laboratory SolutionsDocument4 pagesTesting Services Overview: Advanced Clinical Laboratory SolutionsMalcolm LeeNo ratings yet
- How Does The Thyroid Work? Let's Watch This Video: So Why The Big Commotion Over Such A Small Gland?Document26 pagesHow Does The Thyroid Work? Let's Watch This Video: So Why The Big Commotion Over Such A Small Gland?DrRashmi MenonNo ratings yet
- Functional Medicine Intake Final 07-17-12Document34 pagesFunctional Medicine Intake Final 07-17-12lianaidrisNo ratings yet
- Saudi Guideline Prevention Management Overweight Obesity 2022Document82 pagesSaudi Guideline Prevention Management Overweight Obesity 2022إكرام النايبNo ratings yet
- Constipation Risk Assessment ToolDocument2 pagesConstipation Risk Assessment ToolAnggie Anggriyana100% (1)
- Parkinsons - Management PlanDocument3 pagesParkinsons - Management Planapi-19753815No ratings yet
- Low Carb Food List DownloadDocument1 pageLow Carb Food List Downloadbeth aguirreNo ratings yet
- Rakowski CleanseDocument2 pagesRakowski CleanseBarbara A. Hoffman100% (1)
- Nutrition Consultation FormDocument7 pagesNutrition Consultation FormRD Finders and Personal Training100% (5)
- Rep160417 LLN Rec Eat PlanDocument2 pagesRep160417 LLN Rec Eat PlanANGEL VASILE NICANo ratings yet
- New Developments in The Treatment of Gastroparesis PDFDocument7 pagesNew Developments in The Treatment of Gastroparesis PDFpaulNo ratings yet
- Comprehensive Nursing Assessment For Care Plan: AllergiesDocument14 pagesComprehensive Nursing Assessment For Care Plan: AllergiesBrittany ShrewsburyNo ratings yet
- Blood Interpretation - Functional Medicine - Dr. Adiel Tel-OrenDocument36 pagesBlood Interpretation - Functional Medicine - Dr. Adiel Tel-Orenlokita_opdNo ratings yet
- Toxic Chemicals and WomenDocument6 pagesToxic Chemicals and WomenAlicia Krone100% (1)
- NCP of Patient With GastritisDocument4 pagesNCP of Patient With GastritisBer AnneNo ratings yet
- Genetic Dietetics - Nutrigenomics and The Future of Dietetics PracticeDocument2 pagesGenetic Dietetics - Nutrigenomics and The Future of Dietetics PracticeIffa Karina PermatasariNo ratings yet
- Elimination Diet Food Plan: Dairy Alternatives Proteins Fats & OilsDocument2 pagesElimination Diet Food Plan: Dairy Alternatives Proteins Fats & Oilsd_probst5098No ratings yet
- Aapi Ebook June 19 2017Document621 pagesAapi Ebook June 19 2017AAPIUSANo ratings yet
- Start Low and Go Slow 1-21-2014Document5 pagesStart Low and Go Slow 1-21-2014Ed JonesNo ratings yet
- Blood Chemistry Test Values and Clinical SignificanceDocument3 pagesBlood Chemistry Test Values and Clinical SignificanceHal Theodore Maranian BallotaNo ratings yet
- 7 Daily Habits Hormone Balancing Cheat Sheet Opt inDocument7 pages7 Daily Habits Hormone Balancing Cheat Sheet Opt inLikhita100% (1)
- The Terror of Pediatric Medicine DR SircusDocument338 pagesThe Terror of Pediatric Medicine DR SircusJustiniano Delfin100% (2)
- Food Matters Food Additives To AvoidDocument1 pageFood Matters Food Additives To AvoidPopescu Bogdan ConstantinNo ratings yet
- Milk Allergy M List Hidden NamesDocument2 pagesMilk Allergy M List Hidden NamesNalah Guhrl100% (1)
- The Easy Anti IBS DietDocument23 pagesThe Easy Anti IBS DietDragana ZagorcicNo ratings yet
- Provita WS18 CatalogueDocument87 pagesProvita WS18 CatalogueSorinNo ratings yet
- Food Nutrition Cooking Gold CoastDocument64 pagesFood Nutrition Cooking Gold CoastMartin MatthewsNo ratings yet
- Pet Parents Handbook For Keto and Canine CancerDocument33 pagesPet Parents Handbook For Keto and Canine CancerMeloonNo ratings yet
- Leaky Gut TreatmentDocument5 pagesLeaky Gut Treatmentfsilassie8012No ratings yet
- Prebiotic Effect in The Healthy Infant - Recent Update: Yvan - Vandenplas@uzbrussel - BeDocument53 pagesPrebiotic Effect in The Healthy Infant - Recent Update: Yvan - Vandenplas@uzbrussel - BegazalidjawadNo ratings yet
- Liver Function Testing PDFDocument2 pagesLiver Function Testing PDFRajesh KumarNo ratings yet
- Natural Supplements Brochure 2015Document8 pagesNatural Supplements Brochure 2015Philip ScofieldNo ratings yet
- H&PEDocument2 pagesH&PEDanielleNo ratings yet
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDocument2 pagesDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- Anti Inflammatory DietDocument6 pagesAnti Inflammatory DietHW GomarNo ratings yet
- Breast Pain - History TakingDocument6 pagesBreast Pain - History TakingValencia FooNo ratings yet
- FM SchoolsDocument11 pagesFM SchoolsJeremy ChristmannNo ratings yet
- Nutrition For Cancer Patients During Treatment Part 2Document10 pagesNutrition For Cancer Patients During Treatment Part 2reading4chNo ratings yet
- Antiaging 101: Course Manual: A Proactive Preventive Health Care ProgramFrom EverandAntiaging 101: Course Manual: A Proactive Preventive Health Care ProgramNo ratings yet
- Preconception nutrition for common conditionsDocument26 pagesPreconception nutrition for common conditionsAinie WahidahNo ratings yet
- Untitled BibliographyDocument1 pageUntitled BibliographyAndrew HuaNo ratings yet
- Clinical Cases in Acid Base Imbalance by Dr. Kashif AhmadDocument4 pagesClinical Cases in Acid Base Imbalance by Dr. Kashif AhmadAndrew HuaNo ratings yet
- History 2015-03-27Document1 pageHistory 2015-03-27Andrew HuaNo ratings yet
- Gator Mathematics Competition 2013 Tests and SolutionsDocument24 pagesGator Mathematics Competition 2013 Tests and SolutionsAndrew Hua100% (1)
- Raven Spiral GuideDocument92 pagesRaven Spiral Guidealgo990% (1)
- 2 Periodic MaintenanceDocument35 pages2 Periodic Maintenancestevecrume3435No ratings yet
- HW 3Document6 pagesHW 3Andrew HuaNo ratings yet
- Batzer and Deininger 2002 Nature Reviews GeneticsDocument11 pagesBatzer and Deininger 2002 Nature Reviews GeneticsAndrew HuaNo ratings yet
- BHS Lec 1Document55 pagesBHS Lec 1AtiaNo ratings yet
- DwarfismDocument25 pagesDwarfismTubocurareNo ratings yet
- The Year Of The Yin Fire Pig - Key Events And Predictions For 2019Document3 pagesThe Year Of The Yin Fire Pig - Key Events And Predictions For 2019ay2004janNo ratings yet
- ABG WorksheetDocument10 pagesABG WorksheetRacquel PinnockNo ratings yet
- Guava Intro 1Document4 pagesGuava Intro 1Thean MendozaNo ratings yet
- Preparing For The Coming Influenza PandemicDocument34 pagesPreparing For The Coming Influenza Pandemic1n1No ratings yet
- Drug Study Ciprofloxacin QuinosynDocument10 pagesDrug Study Ciprofloxacin QuinosynNelle ReyNo ratings yet
- Fastidious Gram Negative RodsDocument74 pagesFastidious Gram Negative RodsMaria ClaraNo ratings yet
- Canine and Feline Mega EsophagusDocument10 pagesCanine and Feline Mega Esophagustaner_soysurenNo ratings yet
- Renal Siadh Di CSWDocument54 pagesRenal Siadh Di CSWRizka Nurul Firdaus100% (1)
- The Asphalt DiariesDocument162 pagesThe Asphalt DiariesJames CassarNo ratings yet
- ATORVASTATINDocument1 pageATORVASTATINSHEILA MAE SACLOTNo ratings yet
- Matary Surgical JarsDocument199 pagesMatary Surgical JarsRaouf Ra'fat SolimanNo ratings yet
- MSDS Reach Potassium Silico FluorideDocument6 pagesMSDS Reach Potassium Silico Fluoridesamir5yNo ratings yet
- Pediatric NeurologyDocument24 pagesPediatric NeurologyAndika GhifariNo ratings yet
- Pioped PDFDocument7 pagesPioped PDFaiNo ratings yet
- Pantoea Agglomerans - ADocument9 pagesPantoea Agglomerans - AmadelaineNo ratings yet
- Mutation and Sickle CellDocument16 pagesMutation and Sickle Cellapi-309893409No ratings yet
- Day 9 ASSIGNMENT SDDocument3 pagesDay 9 ASSIGNMENT SDashwinNo ratings yet
- Case Study ExampleDocument25 pagesCase Study ExampleKing Mark MartinezNo ratings yet
- Ascaris LumbricoidesDocument21 pagesAscaris Lumbricoideschocoholic potchiNo ratings yet
- Fs11 Environmental and Genetic InteractionsDocument3 pagesFs11 Environmental and Genetic InteractionsYuliandini Pangestika WiyonoNo ratings yet
- Mental HealthDocument16 pagesMental HealthFaaray Asif100% (1)
- Gastroenteritis in Children: Prepared by R. J. C. Manalo, BSN, RN, MNDocument45 pagesGastroenteritis in Children: Prepared by R. J. C. Manalo, BSN, RN, MNHui ChenNo ratings yet
- Surgery Morning Report FracturesDocument24 pagesSurgery Morning Report FracturesAulia Kurnia FananiNo ratings yet
- 4.4 Shalakya Tantra SyllabusDocument15 pages4.4 Shalakya Tantra SyllabusIshwari GaikwadNo ratings yet
- Modern Review of Dysuria: Causes, Symptoms and ManagementDocument19 pagesModern Review of Dysuria: Causes, Symptoms and ManagementKrishnaNo ratings yet
- Drug Study NCP SoapieDocument15 pagesDrug Study NCP Soapiemikrobyo_ng_wmsuNo ratings yet
- Republic of The Philippines Schools Division of Taguig City and PaterosDocument3 pagesRepublic of The Philippines Schools Division of Taguig City and PaterosArianne B. CabañezNo ratings yet