You might also like
- The Acute NeurologiDocument343 pagesThe Acute Neurologizee zeeNo ratings yet
- Emotional Freedom Techniques and Body Energy HealingDocument45 pagesEmotional Freedom Techniques and Body Energy Healingsonetless100% (2)
- Pediatric Neurology - Pediatric Epilepsy SyndromeDocument6 pagesPediatric Neurology - Pediatric Epilepsy Syndromemkct111100% (1)
- 14 15 Little Red Book of NeurologyDocument117 pages14 15 Little Red Book of NeurologyeloyNo ratings yet
- Neuroscience Ii: Summary: Nationality (Will Tell You Incidence, For Example, AsiansDocument29 pagesNeuroscience Ii: Summary: Nationality (Will Tell You Incidence, For Example, AsiansAngelaTrinidad100% (2)
- Neurology NotesDocument31 pagesNeurology NotesArif Setyawan75% (4)
- Tutor Neurological Examination ..Pocket Tutor.. 2nd Edition 2017 PDFDocument216 pagesTutor Neurological Examination ..Pocket Tutor.. 2nd Edition 2017 PDFsun sealNo ratings yet
- Acute Ataxia in Children: Practice GapsDocument14 pagesAcute Ataxia in Children: Practice Gapsalain reyes100% (1)
- Neurology Made Easy FinalDocument18 pagesNeurology Made Easy FinalDevin Swanepoel100% (1)
- Pediatric Genetics NotesDocument96 pagesPediatric Genetics Noteskkkssbb100% (1)
- MmmGiuseppe Micieli, Anna Cavallini, Stefano Ricci, Domenico Consoli, Jonathan A. Edlow - Decision Algorithms For Emergency Neurology-Springer (2021)Document631 pagesMmmGiuseppe Micieli, Anna Cavallini, Stefano Ricci, Domenico Consoli, Jonathan A. Edlow - Decision Algorithms For Emergency Neurology-Springer (2021)Bulbucan Iulia-Denisa0% (1)
- Pediatric NotesDocument45 pagesPediatric NoteskkkssbbNo ratings yet
- Merrits 13thDocument2,669 pagesMerrits 13th星拉斐100% (3)
- Pediatric Neurology - Lawson Peter N. (SRG)Document200 pagesPediatric Neurology - Lawson Peter N. (SRG)Hriday DeNo ratings yet
- Pediatric Cardiology EvaluationsDocument30 pagesPediatric Cardiology EvaluationsZahra AlaradiNo ratings yet
- Benefits of TriphalaDocument4 pagesBenefits of TriphalaAditya Sharma100% (1)
- Monthly Wellness Tip Heat StressDocument1 pageMonthly Wellness Tip Heat StressbharathaninNo ratings yet
- Cerebral PalsyDocument80 pagesCerebral PalsyYuusuf MubarikNo ratings yet
- Clinical Pediatric NeurologyDocument372 pagesClinical Pediatric NeurologyIntan Leonita50% (2)
- NeurologyDocument118 pagesNeurologykep1313No ratings yet
- Top 5 Auriculotherapy ChartsDocument17 pagesTop 5 Auriculotherapy Chartsmaria100% (2)
- Neurology TipsDocument455 pagesNeurology TipsAsad Khan KhalilNo ratings yet
- The Comprehensive Evaluation and Treatment of Epilepsy: A Practical GuideFrom EverandThe Comprehensive Evaluation and Treatment of Epilepsy: A Practical GuideNo ratings yet
- Physical Therpay Protocols For Conditions of Neck RegionDocument74 pagesPhysical Therpay Protocols For Conditions of Neck Regionjrpsaavedra4599No ratings yet
- Pediatric Neurological Exam ChecklistDocument6 pagesPediatric Neurological Exam ChecklistMai HunnyNo ratings yet
- Fever: Anca Ba Cârea, Alexandru SchiopuDocument24 pagesFever: Anca Ba Cârea, Alexandru SchiopuAndika GhifariNo ratings yet
- MGH Handbook of Neurology 2ndDocument355 pagesMGH Handbook of Neurology 2nddoctorhousemedNo ratings yet
- Spinocerebellar AtaxiasDocument50 pagesSpinocerebellar AtaxiasAshish DuggalNo ratings yet
- Pediatric Hematology-Oncology Ward Officers HandbookDocument78 pagesPediatric Hematology-Oncology Ward Officers HandbookMarcela Catalina Fandiño VargasNo ratings yet
- Pediatric Cardiology Summary TableDocument1 pagePediatric Cardiology Summary TableDarnell DelgadoNo ratings yet
- BrochureDocument6 pagesBrochureNikita JacobsNo ratings yet
- Practical Algorithms in Pediatric Gastroenterology: EditorDocument116 pagesPractical Algorithms in Pediatric Gastroenterology: EditorandresNo ratings yet
- Promoting Neurosciences with Motor Stereotypies and Kluver-Bucy SyndromeDocument3 pagesPromoting Neurosciences with Motor Stereotypies and Kluver-Bucy SyndromewardahkhattakNo ratings yet
- Neurologic Clinics Pediatric Neurology Part IDocument296 pagesNeurologic Clinics Pediatric Neurology Part IPirokunNo ratings yet
- Migraine Headache: in Partial Fulfillment of Nursing 505B by Melissa A. MakhoulDocument26 pagesMigraine Headache: in Partial Fulfillment of Nursing 505B by Melissa A. MakhoulMelissa MakhoulNo ratings yet
- Manual of Pediatric NeurologyDocument148 pagesManual of Pediatric NeurologyannisanangNo ratings yet
- Brainstem MnemonicsDocument2 pagesBrainstem MnemonicsFajar Rudy Qimindra100% (4)
- Neurology Clerkship Study GuideDocument84 pagesNeurology Clerkship Study GuideHilary Steele100% (1)
- Pediatric Neurology - Essentials For General PracticeDocument352 pagesPediatric Neurology - Essentials For General Practiceashrafholail100% (1)
- Medical-Surgical Nursing The Neurologic Concepts: Jimmellee Ellen P. Olilang, RNDocument225 pagesMedical-Surgical Nursing The Neurologic Concepts: Jimmellee Ellen P. Olilang, RNKatrina Sarah Mae MabasaNo ratings yet
- Fenichel Neonatal Neurology Fourth EditionDocument232 pagesFenichel Neonatal Neurology Fourth Editionnaseeruddin04100% (4)
- Handbook of Pediatric Epilepsy: David C. DredgeDocument256 pagesHandbook of Pediatric Epilepsy: David C. DredgeDiana HereldNo ratings yet
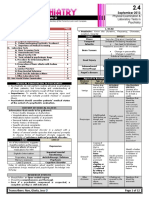
- 02.04. Physical Examination and Laboratory Tests in PsychiatryDocument12 pages02.04. Physical Examination and Laboratory Tests in PsychiatryMiguel C. DolotNo ratings yet
- Bickerstaff Neurological ExaminationDocument73 pagesBickerstaff Neurological ExaminationHisham Elkilaney67% (6)
- Pediatric Myelination and LeukodystrophiesDocument41 pagesPediatric Myelination and LeukodystrophiesAna Bărdaș-ZugravuNo ratings yet
- Libro Electrolitos Segunda EdicionDocument256 pagesLibro Electrolitos Segunda Edicionrodrigo barreraNo ratings yet
- SCE Neurology Web Questions Updated Nov-17Document125 pagesSCE Neurology Web Questions Updated Nov-17Areeb Rauf0% (1)
- Algorithms in Pediatric NeurologyDocument84 pagesAlgorithms in Pediatric NeurologyapheatNo ratings yet
- NefroDocument527 pagesNefroIrina Triboi100% (2)
- NICE Guidlines 2022 Epilepsies in Children Young People and Adults PDFDocument139 pagesNICE Guidlines 2022 Epilepsies in Children Young People and Adults PDFGabriela WidjajaNo ratings yet
- MRI in Stroke PDFDocument281 pagesMRI in Stroke PDFRifqi UlilNo ratings yet
- Child Neurology: Dr. Endang Mutiawati SP.SDocument28 pagesChild Neurology: Dr. Endang Mutiawati SP.SacutdevyNo ratings yet
- Pediatric Epilepsy in Indonesia: With 4 Dimensions Epilepsy ClassificationDocument64 pagesPediatric Epilepsy in Indonesia: With 4 Dimensions Epilepsy ClassificationYahya Taqiuddin RobbaniNo ratings yet
- Ch. Neurology (7th Ed.)Document1,506 pagesCh. Neurology (7th Ed.)Giorgos KarvelasNo ratings yet
- Pediatric NeurologyDocument149 pagesPediatric Neurologyannyzhuk100% (2)
- Differential Diagnosis of Cherry-Red Spot at MaculaDocument4 pagesDifferential Diagnosis of Cherry-Red Spot at MaculaVarun BoddulaNo ratings yet
- Reversing Cerebral Palsy in Early Infancy: A Protocol for Using Normalization Through Neuroplastic Manipulation (NTNM)From EverandReversing Cerebral Palsy in Early Infancy: A Protocol for Using Normalization Through Neuroplastic Manipulation (NTNM)No ratings yet
- Aicardi’s Diseases of the Nervous System in Childhood, 4th EditionFrom EverandAicardi’s Diseases of the Nervous System in Childhood, 4th EditionAlexis ArzimanoglouNo ratings yet
- Acute Disseminated EncephalitisDocument16 pagesAcute Disseminated EncephalitisDedy SavradinataNo ratings yet
- Clinical Pearls in Pediatric CardiologyDocument8 pagesClinical Pearls in Pediatric CardiologySunjon JondhleNo ratings yet
- Swaimans Pediatric Neurology 5edDocument2 pagesSwaimans Pediatric Neurology 5edjaiswalnilesh5132No ratings yet
- Diarrhea (Ped) DDX - Gastroenteritis - Food Poisoning - Uti - Uri - Cow Milk Protein Allergy Dopcsfaaa AbcoDocument34 pagesDiarrhea (Ped) DDX - Gastroenteritis - Food Poisoning - Uti - Uri - Cow Milk Protein Allergy Dopcsfaaa AbcofeawefNo ratings yet
- RefDocument1 pageRefAndika GhifariNo ratings yet
- Ventricular Shunting ProceduresDocument22 pagesVentricular Shunting ProceduresAndika GhifariNo ratings yet
- TAB【Digimon Adventure Tri】-【Butterfly!】MusicGDocument3 pagesTAB【Digimon Adventure Tri】-【Butterfly!】MusicGAndika GhifariNo ratings yet
- Background, Objectives, and OutcomesDocument1 pageBackground, Objectives, and OutcomesAndika GhifariNo ratings yet
- Date and PlaceDocument1 pageDate and PlaceAndika GhifariNo ratings yet
- Bebas Neue - SIL Open Font License 1.1Document4 pagesBebas Neue - SIL Open Font License 1.1SiswantoBudiNo ratings yet
- LicenseDocument1 pageLicenseAndika GhifariNo ratings yet
- RefDocument1 pageRefAndika GhifariNo ratings yet
- Acl PDFDocument2 pagesAcl PDFAndika GhifariNo ratings yet
- 114 - Genetic Origins of Brain TumorsDocument10 pages114 - Genetic Origins of Brain TumorsAndika GhifariNo ratings yet
- Acl PDFDocument2 pagesAcl PDFAndika GhifariNo ratings yet
- Leptospirosis Pada Hewan Dan ManusiaDocument7 pagesLeptospirosis Pada Hewan Dan ManusiaAndika GhifariNo ratings yet
- Leptospirosis - Ferri's Clinical AdvisorDocument2 pagesLeptospirosis - Ferri's Clinical AdvisorAndika GhifariNo ratings yet
- Leptospirosis - Ferri's Clinical AdvisorDocument2 pagesLeptospirosis - Ferri's Clinical AdvisorAndika GhifariNo ratings yet
- Isokinetic Torque, Flexion/Extension Average Ratios in Power, and Nondisabled Adults and Adults With Mental RetardationDocument5 pagesIsokinetic Torque, Flexion/Extension Average Ratios in Power, and Nondisabled Adults and Adults With Mental RetardationAndika GhifariNo ratings yet
- AnnouncementDocument20 pagesAnnouncementAndika GhifariNo ratings yet
- Dafpus Lama ReferatDocument2 pagesDafpus Lama ReferatAndika GhifariNo ratings yet
- Replikasi of DNADocument49 pagesReplikasi of DNAAndika Ghifari0% (1)
- LicenseDocument13 pagesLicensekarlaNo ratings yet
- Childhood ImmunisationDocument6 pagesChildhood ImmunisationAndika GhifariNo ratings yet
- EXP CoverSheetDocument3 pagesEXP CoverSheetAndika GhifariNo ratings yet
- Health Psychology Migraine ProjectDocument46 pagesHealth Psychology Migraine Projectwajiha yaminNo ratings yet
- Conium Maculatum: Common Name: Prover: FamilyDocument4 pagesConium Maculatum: Common Name: Prover: FamilySuhas IngaleNo ratings yet
- When A Migraine OccurDocument9 pagesWhen A Migraine OccurKARL PASCUANo ratings yet
- Hubungan Kualitas Tidur Dengan Jenis Nyeri Kepala Primer Pada Siswa-Siswi Sma Negeri 1 PadangDocument10 pagesHubungan Kualitas Tidur Dengan Jenis Nyeri Kepala Primer Pada Siswa-Siswi Sma Negeri 1 PadangAghie vlogNo ratings yet
- Neurologic Involvement in Scleroderma, A Systematic ReviewDocument13 pagesNeurologic Involvement in Scleroderma, A Systematic ReviewIsa RahmatikawatiNo ratings yet
- Urografin Urografin 76Document8 pagesUrografin Urografin 76KartikGachinmaniNo ratings yet
- Cause Effect ParagraphDocument4 pagesCause Effect ParagraphZineb AmelNo ratings yet
- Icd-10-Cm Coding Guidance For Traumatic Brain Injury: Medical Provider Screening and Diagnostic Coding Dod Tbi DefinitionDocument3 pagesIcd-10-Cm Coding Guidance For Traumatic Brain Injury: Medical Provider Screening and Diagnostic Coding Dod Tbi DefinitionchaandNo ratings yet
- Chapter 46: Neurologic Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument5 pagesChapter 46: Neurologic Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Guide to the Head and Neck ChapterDocument87 pagesGuide to the Head and Neck ChapterGuia De GuzmanNo ratings yet
- Mitanin Study FINALDocument37 pagesMitanin Study FINALAshok DadasNo ratings yet
- Skin DiseasesDocument33 pagesSkin DiseasesKir Kal KarNo ratings yet
- Evaluation of Headache in AdultsDocument21 pagesEvaluation of Headache in AdultsMaicon RamosNo ratings yet
- 04 Taking A Case HistoryDocument38 pages04 Taking A Case HistoryMwanja MosesNo ratings yet
- IJRPR1370Document9 pagesIJRPR1370Dèv ThãkürNo ratings yet
- Herniation of Uncus and Parahippocampal Gyrus: An Accidental Finding On Magnetic Resonance Imaging of CerebrumDocument3 pagesHerniation of Uncus and Parahippocampal Gyrus: An Accidental Finding On Magnetic Resonance Imaging of CerebrumDanaAmaranducaiNo ratings yet
- Practical Book of TherapeuticsDocument28 pagesPractical Book of TherapeuticsSara AbdoNo ratings yet
- IPK - Pengantar PBL (Swamedikasi)Document30 pagesIPK - Pengantar PBL (Swamedikasi)Riani LetelayNo ratings yet
- H. Gremillion-Temporomandibular Disorders and Orafacial Pain, An Issue of Dental Clinics (The Clinics - Dentistry) - Saunders (2007) PDFDocument274 pagesH. Gremillion-Temporomandibular Disorders and Orafacial Pain, An Issue of Dental Clinics (The Clinics - Dentistry) - Saunders (2007) PDFSamuel Flores CalderonNo ratings yet
- Does Klonopin (Clonazepam) Work For MigrainesDocument4 pagesDoes Klonopin (Clonazepam) Work For MigrainesTooba SiddiquiNo ratings yet
- Reading Test - 3 Clinical Depression Text ADocument17 pagesReading Test - 3 Clinical Depression Text AJisha JanardhanNo ratings yet
- Red Flags ArticleDocument4 pagesRed Flags ArticleINNOCENT KHULIWANo ratings yet