You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lesson 5.1 Worksheets (1) COMPLETEDocument6 pagesLesson 5.1 Worksheets (1) COMPLETEBrianna Dominguez50% (6)
- MAS-42F (Relevant Costing With Linear Programming)Document9 pagesMAS-42F (Relevant Costing With Linear Programming)Pearl Mae De VeasNo ratings yet
- What Is The Difference Between The Hardness, Toughness, Resilience, and Stiffness of Materials - QuoraDocument5 pagesWhat Is The Difference Between The Hardness, Toughness, Resilience, and Stiffness of Materials - QuoraUdit AgarwalNo ratings yet
- Chapter 14. Intestinal GasDocument19 pagesChapter 14. Intestinal GasMonica CiorneiNo ratings yet
- Collecting and Exhibiting Tree LeavesDocument4 pagesCollecting and Exhibiting Tree LeavesChuck AchbergerNo ratings yet
- HRM - EssayDocument17 pagesHRM - EssayvsnaveenkNo ratings yet
- Chapter 9 - The School Head in School-Based Management (SBM)Document22 pagesChapter 9 - The School Head in School-Based Management (SBM)Myla GuabNo ratings yet
- Laparoscopic AppendectomyDocument24 pagesLaparoscopic AppendectomyMosher MundaNo ratings yet
- Report Information From Proquest: 21 January 2014 08:58Document4 pagesReport Information From Proquest: 21 January 2014 08:58Elizar JarNo ratings yet
- ProQuestDocuments 2014 01 21Document4 pagesProQuestDocuments 2014 01 21Elizar JarNo ratings yet
- ProQuestDocuments 2014 01 21Document4 pagesProQuestDocuments 2014 01 21Elizar JarNo ratings yet
- Report Information From Proquest: 21 January 2014 09:01Document4 pagesReport Information From Proquest: 21 January 2014 09:01Elizar JarNo ratings yet
- ProQuestDocuments 2014 01 21Document4 pagesProQuestDocuments 2014 01 21Elizar JarNo ratings yet
- ProQuestDocuments 2014 01 21Document4 pagesProQuestDocuments 2014 01 21Elizar JarNo ratings yet
- ProQuestDocuments 2014 01 21Document6 pagesProQuestDocuments 2014 01 21Elizar JarNo ratings yet
- Control 508Document31 pagesControl 508Elizar JarNo ratings yet
- Lecture AppendicitisDocument29 pagesLecture AppendicitisWito Eka PutraNo ratings yet
- Appendicitis and PeritonitisDocument22 pagesAppendicitis and PeritonitisElizar JarNo ratings yet
- Guidelines For Adult Diabetes (DM) Care: Abc'SDocument2 pagesGuidelines For Adult Diabetes (DM) Care: Abc'SElizar JarNo ratings yet
- Likelihood That A Woman Will Have No Major Risk Factors at The Time of First Myocardial Infarction or StrokeDocument4 pagesLikelihood That A Woman Will Have No Major Risk Factors at The Time of First Myocardial Infarction or StrokeElizar JarNo ratings yet
- Stroke:: Remember The 1st Three Letters...Document3 pagesStroke:: Remember The 1st Three Letters...Elizar JarNo ratings yet
- Date: 05/11/2023: Dear Sir/MadamDocument8 pagesDate: 05/11/2023: Dear Sir/MadamMohammad Ali ArianNo ratings yet
- Jan 13 2018Document20 pagesJan 13 2018Jenna MWNo ratings yet
- Ezekiel, The Prophet of The ExileDocument10 pagesEzekiel, The Prophet of The ExileSung RemiNo ratings yet
- WHO 2018 Health at A Glance Mortality Asia Pac Region OctoberDocument3 pagesWHO 2018 Health at A Glance Mortality Asia Pac Region Octoberbiko97jcjNo ratings yet
- Case Study:-Grahak Telecom Summary:-: Human Resources Management Assignment - IiiDocument3 pagesCase Study:-Grahak Telecom Summary:-: Human Resources Management Assignment - IiiRaj ChauhanNo ratings yet
- Review Lesson 11: Caring For Pets at Home: Quarter 1 Week 4 Day 2 SEP. 20-24 E.P.P.4-Agriculture ArtsDocument8 pagesReview Lesson 11: Caring For Pets at Home: Quarter 1 Week 4 Day 2 SEP. 20-24 E.P.P.4-Agriculture ArtsPaulo MalazarteNo ratings yet
- PDFDocument595 pagesPDFKharisma PratamaNo ratings yet
- Learning Packet: Practical Research 1Document9 pagesLearning Packet: Practical Research 1takamiya nahoNo ratings yet
- Sri Kumaran Children's Home - CBSE: I. Circle The Correct AnswerDocument3 pagesSri Kumaran Children's Home - CBSE: I. Circle The Correct AnswersaanviNo ratings yet
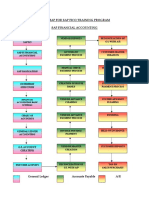
- Roadmap For SAP FICO Training ProgramDocument4 pagesRoadmap For SAP FICO Training ProgramCorpsalesNo ratings yet
- Magnetic Effect of Electric Current PortfolioDocument3 pagesMagnetic Effect of Electric Current PortfolioAshish KumarNo ratings yet
- A Maternal and Child's Nurses Quest Towards ExcellenceDocument78 pagesA Maternal and Child's Nurses Quest Towards Excellencedecsag06No ratings yet
- Project Report On Worker Turnover On KDS GarmentsDocument18 pagesProject Report On Worker Turnover On KDS GarmentsShelveyElmoDiasNo ratings yet
- Allie Brown: Southern Paws Pet Grooming, Cordele, GA. - BatherDocument2 pagesAllie Brown: Southern Paws Pet Grooming, Cordele, GA. - Batherapi-548153301No ratings yet
- Typical Interview Questions (6-8 Questions) : Visa QuestionnaireDocument2 pagesTypical Interview Questions (6-8 Questions) : Visa QuestionnaireSupriya CoolNo ratings yet
- S2-1 Caso Distribución Chocolate Market SoniaDocument2 pagesS2-1 Caso Distribución Chocolate Market SoniasoniaNo ratings yet
- Outdoor Lighting Catalogue - CompressedDocument34 pagesOutdoor Lighting Catalogue - CompressedKamugasha KagonyeraNo ratings yet
- Diesel Engine BasicsDocument11 pagesDiesel Engine BasicsmelissaNo ratings yet
- Eco261 Banking IndustryDocument25 pagesEco261 Banking IndustryAHMAD FILZA ADIRANo ratings yet
- Agenda Myp Cat 1 SciencesDocument1 pageAgenda Myp Cat 1 Sciencesapi-308447912No ratings yet
- MIS Template EditingDocument31 pagesMIS Template Editingesmaadrian18No ratings yet
- Security Analysis (Mauboussin) SP2015Document12 pagesSecurity Analysis (Mauboussin) SP2015Glaiza OrtigueroNo ratings yet
- Ideology: Teun A. Van DijkDocument11 pagesIdeology: Teun A. Van Dijkkim whiteNo ratings yet