You might also like
- 3.9 SOP Internal Audit v1Document11 pages3.9 SOP Internal Audit v1Pramod AthiyarathuNo ratings yet
- Monastery of The Seven Rays - Year 1Document193 pagesMonastery of The Seven Rays - Year 1Lykathea Harmony Pax100% (5)
- Internal Audit SOPDocument4 pagesInternal Audit SOPIftikhar Khan100% (1)
- 'Account StatementDocument11 pages'Account StatementSikander Qazi100% (2)
- All About AvanadeDocument16 pagesAll About AvanadeSunil PatidarNo ratings yet
- Internal Quality Audit ProcedureDocument3 pagesInternal Quality Audit ProcedureAcholonu Emeka Jp100% (2)
- Sample Management Review ChecklistDocument4 pagesSample Management Review Checklistpoetoet100% (1)
- QMS 010 Classification Definition and Approval Matrix of GMP Documents SampleDocument5 pagesQMS 010 Classification Definition and Approval Matrix of GMP Documents SampleRosella Planta100% (1)
- Internal Audit SOPDocument2 pagesInternal Audit SOPNazmun100% (3)
- Q2-760-01-Control of Monitoring and Measuring DevicesDocument5 pagesQ2-760-01-Control of Monitoring and Measuring DevicesAlineNo ratings yet
- Stock VerificationDocument11 pagesStock Verificationrockyrr100% (1)
- QMS 065 SampleDocument6 pagesQMS 065 SamplebaluchakpNo ratings yet
- Internal Audit ISO 9001-2008 Checklist 1-20-12Document43 pagesInternal Audit ISO 9001-2008 Checklist 1-20-12TravisNo ratings yet
- VMware vSAN Network Design PDFDocument169 pagesVMware vSAN Network Design PDFFederico MiliaccaNo ratings yet
- Star Magazine - 18 November 2013Document74 pagesStar Magazine - 18 November 2013LouieLongNeckNo ratings yet
- AM-QMS-05-Internal Quality Audit Procedure - Ver 1Document6 pagesAM-QMS-05-Internal Quality Audit Procedure - Ver 1Deepan TravellerNo ratings yet
- InternalAuditSOP 012413Document8 pagesInternalAuditSOP 012413zubair90No ratings yet
- QSP 02 - Record Control ProcedureDocument5 pagesQSP 02 - Record Control ProcedureVivek V100% (1)
- ESCL-SOP-018, Inspection and Test Procedure For Egba Split-ClampsDocument6 pagesESCL-SOP-018, Inspection and Test Procedure For Egba Split-ClampsadiqualityconsultNo ratings yet
- Competency SOPDocument10 pagesCompetency SOPD Tech Dental Technologies100% (1)
- QP-004 Management Review ProcessDocument3 pagesQP-004 Management Review Processesraa asemNo ratings yet
- ISO 13485 PurchasingDocument5 pagesISO 13485 PurchasingSubhashNo ratings yet
- Example of An Internal Audit SOPDocument3 pagesExample of An Internal Audit SOPVeronica Sebald100% (1)
- Quality Assurance (QA) Management Procedures: By: Pharma Tips - Views: 14415 - Date: 06-May-2012Document6 pagesQuality Assurance (QA) Management Procedures: By: Pharma Tips - Views: 14415 - Date: 06-May-2012SrinivasNo ratings yet
- Sop (Internal Audit)Document6 pagesSop (Internal Audit)Arijit Pattanayak100% (2)
- Minutes of Management Review Meeting OkDocument3 pagesMinutes of Management Review Meeting Okdidar100% (4)
- Internal Audit ProcedureDocument1 pageInternal Audit ProcedureXi MoNo ratings yet
- Form IA-002A (Audit Plan) (07-13-2012)Document2 pagesForm IA-002A (Audit Plan) (07-13-2012)granburyjohnstevens100% (1)
- Procedure For Preventive ActionDocument6 pagesProcedure For Preventive ActionHamzah Abbass Sibai100% (1)
- Sample SOP of Internal Audit of A ProcessDocument10 pagesSample SOP of Internal Audit of A Processsarvjeet_kaushalNo ratings yet
- Document Control Effectiveness in ISO 15189 Accredited LaboratoriesDocument12 pagesDocument Control Effectiveness in ISO 15189 Accredited LaboratoriesinventionjournalsNo ratings yet
- Internal Audit Planning and Scheduling Sample FormatDocument3 pagesInternal Audit Planning and Scheduling Sample Formatsameh100% (2)
- Sop PurchasingDocument5 pagesSop PurchasingSteven TanNo ratings yet
- Internal Audit ProceduresDocument15 pagesInternal Audit ProceduresTait G MafuraNo ratings yet
- Iso22000 - Internal Audit ChecklistDocument2 pagesIso22000 - Internal Audit ChecklistGidion Jeffri PoerbaNo ratings yet
- Auditee Feedback Form: Internal Audit DepartmentDocument2 pagesAuditee Feedback Form: Internal Audit DepartmentNiomi GolraiNo ratings yet
- SOP-03 (Employee Performance Monitoring)Document6 pagesSOP-03 (Employee Performance Monitoring)FarhanNo ratings yet
- QSP 8.3.1 Nonconforming Product - SampleDocument3 pagesQSP 8.3.1 Nonconforming Product - SampleGladys Calvo100% (2)
- Objectives and Goals of Auditing Vendors and Production DepartmentDocument15 pagesObjectives and Goals of Auditing Vendors and Production DepartmentFfwms SpainNo ratings yet
- QP-72-03 Customer CommunicationDocument3 pagesQP-72-03 Customer CommunicationSamsudin AhmadNo ratings yet
- G Corrective Action Section 7Document3 pagesG Corrective Action Section 7Ngonidzashe Zvarevashe100% (1)
- ISODocument11 pagesISOaiswaryacdas9853No ratings yet
- How Can ISO 13485 Clause 7.4, Purchasing, Enhance ProcurementDocument3 pagesHow Can ISO 13485 Clause 7.4, Purchasing, Enhance ProcurementPavan MujawdiyaNo ratings yet
- SOPSP05 VendorSelection BSDocument3 pagesSOPSP05 VendorSelection BStroubledsoul100% (1)
- Quality Management System Master18 February 2014Document27 pagesQuality Management System Master18 February 2014shani5573No ratings yet
- QSP-001633 - Rev 04 - Luminus Testing Laboratory Quality Manual207Document34 pagesQSP-001633 - Rev 04 - Luminus Testing Laboratory Quality Manual207SureshNo ratings yet
- New Supplier Survey FormDocument14 pagesNew Supplier Survey Formsutharitessh100% (1)
- Internal Audit NC ReportDocument1 pageInternal Audit NC Reportmorshed_mahamud7055No ratings yet
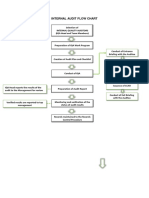
- Internal Audit Flow ChartDocument1 pageInternal Audit Flow ChartstevierayoNo ratings yet
- Evaluation Reporting of ResultsDocument16 pagesEvaluation Reporting of ResultspurnachandrashekarNo ratings yet
- Procedure On Document ManagementDocument13 pagesProcedure On Document Managementndayiragije JMVNo ratings yet
- Internal Quality Audit Plan Dilg Region 10Document8 pagesInternal Quality Audit Plan Dilg Region 10Cess AyomaNo ratings yet
- Process Audit ChecklistDocument15 pagesProcess Audit ChecklistAbi ParillaNo ratings yet
- Control of Monitoring and Measuring EquipmentDocument3 pagesControl of Monitoring and Measuring EquipmentLinda Setya WatiNo ratings yet
- FDA Volume II - Audits Ora-Lab.4.14Document7 pagesFDA Volume II - Audits Ora-Lab.4.14nilayNo ratings yet
- SOP-4.3-2-0 Creation, Revision and Approval of DocumentsDocument4 pagesSOP-4.3-2-0 Creation, Revision and Approval of DocumentsclairealbertiniNo ratings yet
- QMS Internal External AuditDocument5 pagesQMS Internal External AuditNesanNo ratings yet
- Quality AuditsDocument15 pagesQuality AuditsPrachi PandeyNo ratings yet
- SOP-03 Management Review MeetingsDocument3 pagesSOP-03 Management Review Meetingstrivesh100% (1)
- Purchasing PolicyDocument9 pagesPurchasing PolicyAyman AliNo ratings yet
- E 178 Iso17025 ChecklistDocument19 pagesE 178 Iso17025 ChecklistShweta Rawal VijNo ratings yet
- Auditing Gas Analysis LaboratoriesDocument14 pagesAuditing Gas Analysis LaboratorieshentadwyNo ratings yet
- NQA Aerospace Workshop Webinar 02.10.2020Document53 pagesNQA Aerospace Workshop Webinar 02.10.2020Rony LesbtNo ratings yet
- Form JO Foundation ChecklistDocument1 pageForm JO Foundation ChecklistRony LesbtNo ratings yet
- NQA Webinar - Cyber Security Risk and Assurance in The Supply Chain (WMCRC & Tuned To RISK) 21.04.21Document36 pagesNQA Webinar - Cyber Security Risk and Assurance in The Supply Chain (WMCRC & Tuned To RISK) 21.04.21Rony LesbtNo ratings yet
- NQA Webinar PAS 2060 Carbon Neutrality 30-04-2021Document38 pagesNQA Webinar PAS 2060 Carbon Neutrality 30-04-2021Rony LesbtNo ratings yet
- TBM FormDocument1 pageTBM FormRony LesbtNo ratings yet
- Hand Out Shop Inspection - ISBL - OSBL 210527Document3 pagesHand Out Shop Inspection - ISBL - OSBL 210527Rony LesbtNo ratings yet
- Summary RFI of FDT UG PipeDocument2 pagesSummary RFI of FDT UG PipeRony LesbtNo ratings yet
- Cause Analysis For Spun Pile Crack and BrokenDocument11 pagesCause Analysis For Spun Pile Crack and BrokenRony LesbtNo ratings yet
- 35 - HS-78005 - Isolation ProcedureDocument3 pages35 - HS-78005 - Isolation ProcedureRony LesbtNo ratings yet
- DCC-F9 - Format Job DescriptionDocument1 pageDCC-F9 - Format Job DescriptionRony LesbtNo ratings yet
- TgBin TTB B0 HS 78045 Handling SRCC Documentation and DistributionDocument15 pagesTgBin TTB B0 HS 78045 Handling SRCC Documentation and DistributionRony LesbtNo ratings yet
- Course Assessment Form Date .. . Course Title: . Facilitator: Location: .. 1Document1 pageCourse Assessment Form Date .. . Course Title: . Facilitator: Location: .. 1Rony LesbtNo ratings yet
- Name Target # of Abnormality Finding (# of Mudawalk/month) Week 1 Week 2 Week 3Document3 pagesName Target # of Abnormality Finding (# of Mudawalk/month) Week 1 Week 2 Week 3Rony LesbtNo ratings yet
- Register of Operation On ProcessDocument18 pagesRegister of Operation On ProcessRony LesbtNo ratings yet
- Sop Billing ProcessDocument9 pagesSop Billing ProcessRony Lesbt0% (1)
- P-OkiPL1-100-15-PRO-0002 HSE Induction ProcedureDocument14 pagesP-OkiPL1-100-15-PRO-0002 HSE Induction ProcedureRony Lesbt100% (2)
- P OkiPL1 100 15 PRO 0003 Emergency Preparedness and Emergency ResponseDocument13 pagesP OkiPL1 100 15 PRO 0003 Emergency Preparedness and Emergency ResponseRony LesbtNo ratings yet
- Inter Job Handed OverDocument1 pageInter Job Handed OverRony LesbtNo ratings yet
- WI - Interdiscipline Handed OverDocument5 pagesWI - Interdiscipline Handed OverRony LesbtNo ratings yet
- P-OkiPL1-100-15-PRO-0001 Legal and Other Requirements ProcedureDocument11 pagesP-OkiPL1-100-15-PRO-0001 Legal and Other Requirements ProcedureRony LesbtNo ratings yet
- UT Training Schedule Angkatan Ke-11Document1 pageUT Training Schedule Angkatan Ke-11Rony LesbtNo ratings yet
- Jobmigas 19 August 2013Document2 pagesJobmigas 19 August 2013Rony LesbtNo ratings yet
- Training Traveling Targeting: Welding Inspector - BNSP (Saturday and Sunday, 19.00Document2 pagesTraining Traveling Targeting: Welding Inspector - BNSP (Saturday and Sunday, 19.00Rony LesbtNo ratings yet
- IEE STD C37.104-2002 IEEE Guide For Automatic Reclosing PDFDocument55 pagesIEE STD C37.104-2002 IEEE Guide For Automatic Reclosing PDFJohnatan HernándezNo ratings yet
- Ackermannand Chen 2013 Developing Academic Collocation List AuthorsmanuscriptDocument31 pagesAckermannand Chen 2013 Developing Academic Collocation List AuthorsmanuscriptaridNo ratings yet
- DPP 05Document4 pagesDPP 05urmomNo ratings yet
- End of Term 2 Test A: Grammar VocabularyDocument3 pagesEnd of Term 2 Test A: Grammar VocabularyAngela Lobato MañanesNo ratings yet
- Chemical and Mechanical DesignDocument460 pagesChemical and Mechanical DesignNuriman K-monNo ratings yet
- Effects of Operating Parameters On Nitrogen Oxides Emissions For A Natural GasDocument9 pagesEffects of Operating Parameters On Nitrogen Oxides Emissions For A Natural GasMudhafar MudhafarNo ratings yet
- Introduction To PEG (Parsing Expression Grammar) in PythonDocument71 pagesIntroduction To PEG (Parsing Expression Grammar) in Pythonrwanda0% (1)
- Applied Mechanics I - Fall 2013 PDFDocument4 pagesApplied Mechanics I - Fall 2013 PDFRajeshGupta100% (1)
- Question BankDocument13 pagesQuestion BankFirozNo ratings yet
- Kuji in KanjiDocument25 pagesKuji in Kanjidcamu37100% (3)
- Request For TransferDocument3 pagesRequest For TransferDiomedes ColarNo ratings yet
- 20120229000242SMA3013 - Chapter 1Document105 pages20120229000242SMA3013 - Chapter 1Nurul Hana BalqisNo ratings yet
- Textbook PMDocument46 pagesTextbook PMLai QuocNo ratings yet
- Quays: Healy Power Quarries LTDDocument48 pagesQuays: Healy Power Quarries LTDmwmccarthyNo ratings yet
- Analisis Sootblower Terhadap Head TransferDocument5 pagesAnalisis Sootblower Terhadap Head TransferRDSetyawanNo ratings yet
- Product Info WISI-GT-31-W V3.0 enDocument2 pagesProduct Info WISI-GT-31-W V3.0 enDiego MattaNo ratings yet
- Agency Enrollment FormDocument1 pageAgency Enrollment FormRaymond TenchavezNo ratings yet
- Weld Overlay Cladding1Document3 pagesWeld Overlay Cladding1Yetkin ErdoğanNo ratings yet
- Indian Contract ActDocument18 pagesIndian Contract ActShubhi MittalNo ratings yet
- Kissing FishDocument11 pagesKissing FishkohlerfernandaNo ratings yet
- Razr Iron Scorpions MC Series Book 1 Motorcycle Club Mafia Romance Crossover Universe Book 3 Harley Diamond All ChapterDocument66 pagesRazr Iron Scorpions MC Series Book 1 Motorcycle Club Mafia Romance Crossover Universe Book 3 Harley Diamond All Chapterphillip.mesias887100% (5)
- Study Guide Unit 2.2 - Dna Replication & Protein SynthesisDocument35 pagesStudy Guide Unit 2.2 - Dna Replication & Protein SynthesisGraceNo ratings yet
- GRP WRKDocument5 pagesGRP WRKrheaNo ratings yet
- Uploading 8 23Document12 pagesUploading 8 23Shannara21No ratings yet
- WeldingDocument23 pagesWeldingSuneel Kumar MeenaNo ratings yet