You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
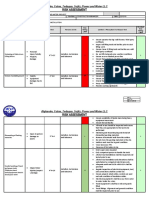
- Risk Assessment For Cable Laying and Raceway InstallationDocument15 pagesRisk Assessment For Cable Laying and Raceway Installationmanikandan100% (3)
- Tail of The Blue Bird by Parkes, Nii AyikweiDocument140 pagesTail of The Blue Bird by Parkes, Nii AyikweiEduardo Crivelli100% (1)
- Short Wave Diathermy Lecture 2013Document69 pagesShort Wave Diathermy Lecture 2013Faisal Qureshi100% (3)
- Republic of The Philippines Central Mindanao University College of Nursing Course OutlineDocument3 pagesRepublic of The Philippines Central Mindanao University College of Nursing Course OutlineEmvie Loyd Pagunsan-ItableNo ratings yet
- Electrode Placement & Functional Movement: Sponsored byDocument28 pagesElectrode Placement & Functional Movement: Sponsored byFaisal Qureshi0% (1)
- St. Patrick's High School: Test Form Morning PrimaryDocument2 pagesSt. Patrick's High School: Test Form Morning PrimaryFaisal QureshiNo ratings yet
- PT Notes: Electrodiagnostic Procedures: Traditional Electrical Evaluation TestsDocument4 pagesPT Notes: Electrodiagnostic Procedures: Traditional Electrical Evaluation TestsFaisal QureshiNo ratings yet
- Microwave Diathermy 2013Document27 pagesMicrowave Diathermy 2013Faisal QureshiNo ratings yet
- Prevalence of Fibromyalgia in Caregiver of Stroke PatientsDocument8 pagesPrevalence of Fibromyalgia in Caregiver of Stroke PatientsFaisal QureshiNo ratings yet
- Standards of Proficiency PhysiotherapistsDocument20 pagesStandards of Proficiency PhysiotherapistsFaisal QureshiNo ratings yet
- Infra Red Radiation Therapy FinalDocument19 pagesInfra Red Radiation Therapy FinalFaisal QureshiNo ratings yet
- HEC Recognized Curriculum For DOctor of Physdiotherapy 2010Document196 pagesHEC Recognized Curriculum For DOctor of Physdiotherapy 2010Faisal QureshiNo ratings yet
- SWD For SinusesDocument9 pagesSWD For SinusesFaisal QureshiNo ratings yet
- A Case Study For Electrical StimulationDocument3 pagesA Case Study For Electrical StimulationFaisal QureshiNo ratings yet
- Petrovsky1 Jar SpringDocument9 pagesPetrovsky1 Jar SpringFaisal QureshiNo ratings yet
- 6 Promoting SafetyDocument30 pages6 Promoting SafetyFaisal QureshiNo ratings yet
- High vs. Low Electrical Stimulation Frequencies For Motor Recovery in HemiplegiaDocument67 pagesHigh vs. Low Electrical Stimulation Frequencies For Motor Recovery in HemiplegiaFaisal QureshiNo ratings yet
- Quantitative Data Analysis PresentationDocument23 pagesQuantitative Data Analysis PresentationFaisal QureshiNo ratings yet
- Excel Lesson 3Document26 pagesExcel Lesson 3Faisal QureshiNo ratings yet
- Effective Vocabulary Activities & Games: Presented by Nicole Castilleja, Mary Kirby and Kathy ThornockDocument27 pagesEffective Vocabulary Activities & Games: Presented by Nicole Castilleja, Mary Kirby and Kathy ThornockFaisal Qureshi100% (1)
- Excel Lesson 5Document28 pagesExcel Lesson 5Faisal QureshiNo ratings yet
- Excel Lesson 2Document27 pagesExcel Lesson 2Faisal QureshiNo ratings yet
- Excel Lesson 3Document26 pagesExcel Lesson 3Faisal QureshiNo ratings yet
- Imp Fire Retardant Test ASTM-D5664-01aDocument2 pagesImp Fire Retardant Test ASTM-D5664-01aangelsfweNo ratings yet
- Coagulants For Water TreatmentDocument48 pagesCoagulants For Water TreatmentClauwie Ganoy BuenavistaNo ratings yet
- HexaflexDocument3 pagesHexaflexfdfdsfasdNo ratings yet
- Aoac 981.16Document2 pagesAoac 981.16Angélica VargasNo ratings yet
- Protection Against Neutron Radiation: CouncilDocument159 pagesProtection Against Neutron Radiation: CouncilFernanda MouraNo ratings yet
- (Backup) Boreas Catalogue1 PDFDocument92 pages(Backup) Boreas Catalogue1 PDFAmyt SrivastavNo ratings yet
- Dost Ki Family or Os Ki GF Ka Sath Part 01 To 41Document15,540 pagesDost Ki Family or Os Ki GF Ka Sath Part 01 To 41Saif KhanzNo ratings yet
- Beaconhouse School System North Nazimabad O Level Commerce Assignment 2 Grade XIDocument11 pagesBeaconhouse School System North Nazimabad O Level Commerce Assignment 2 Grade XIAbdulhadi MushtaqNo ratings yet
- 1st Departmental Test in TLE 7Document2 pages1st Departmental Test in TLE 7jc milNo ratings yet
- Level SwitchDocument2 pagesLevel SwitchIon VairamuthuNo ratings yet
- Affection - Wikipedia, The Free EncyclopediaDocument4 pagesAffection - Wikipedia, The Free EncyclopediaAnonymous ifnQFq42oKNo ratings yet
- Rele Sobretension DPC01DM48Document6 pagesRele Sobretension DPC01DM48LeonardoNo ratings yet
- Gender EqualityDocument11 pagesGender Equalitysquad32mawa2017No ratings yet
- Crop Protection Guide: For Nursery and Landscape PlantsDocument156 pagesCrop Protection Guide: For Nursery and Landscape PlantsAdrian FilipNo ratings yet
- Process Line SizingDocument21 pagesProcess Line Sizingsj_scribdNo ratings yet
- Engro Foods Limited Case StudyDocument5 pagesEngro Foods Limited Case Studymubin_ashraf0% (1)
- I. MULTIPLE CHOICE. Choose The Letter of The Correct Answer. Write Your Answer On The Space Provided BeforeDocument3 pagesI. MULTIPLE CHOICE. Choose The Letter of The Correct Answer. Write Your Answer On The Space Provided Beforejam syNo ratings yet
- Essay On Junk FoodDocument6 pagesEssay On Junk Foodhupkakaeg100% (2)
- Claim Form-Salaam TakafulDocument2 pagesClaim Form-Salaam TakafulNiaz Ali0% (1)
- Tutorial Sheet - 1 On Design of Spring': Department of Mechanical EngineeringDocument2 pagesTutorial Sheet - 1 On Design of Spring': Department of Mechanical EngineeringSrimanthula SrikanthNo ratings yet
- BCMEDocument35 pagesBCMErupanandaNo ratings yet
- vdYoyHdeTKeL7EhJwoXE - Insomnia PH SlidesDocument40 pagesvdYoyHdeTKeL7EhJwoXE - Insomnia PH SlidesKreshnik IdrizajNo ratings yet
- D-Block Elements & F-Block Elements - Theory, Solved Ex. Module-3-2Document26 pagesD-Block Elements & F-Block Elements - Theory, Solved Ex. Module-3-2Raju SinghNo ratings yet
- Faq-Trade LicenseDocument2 pagesFaq-Trade LicenseVandana Ac KapoorNo ratings yet
- Iso 3452 2 2000 en PDFDocument11 pagesIso 3452 2 2000 en PDFPierpaolo AparoNo ratings yet
- Jimma University Collage of Natural Science Department of ChemistryDocument8 pagesJimma University Collage of Natural Science Department of Chemistryfiraol mokonnenNo ratings yet
- "Probability": Arun Kumar, Ravindra Gokhale, and Nagarajan KrishnamurthyDocument53 pages"Probability": Arun Kumar, Ravindra Gokhale, and Nagarajan KrishnamurthyNirmal SasidharanNo ratings yet