You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Historical Development Summary of Automatic Cannon Caliber Ammunition 20-30mm by Dale DavisDocument215 pagesHistorical Development Summary of Automatic Cannon Caliber Ammunition 20-30mm by Dale DavisAmmoResearchNo ratings yet
- Lesson Plan - The Science of Light and ImpressionismDocument10 pagesLesson Plan - The Science of Light and Impressionismapi-317030373No ratings yet
- Introductory Statistics 2nd Edition Gould Test BankDocument21 pagesIntroductory Statistics 2nd Edition Gould Test Bankodilemelanie83au100% (31)
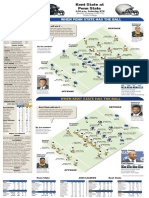
- Kent State at Penn StateDocument1 pageKent State at Penn StatedlevarseNo ratings yet
- South Yarra Cable Tram Engine House and Tram ShedDocument18 pagesSouth Yarra Cable Tram Engine House and Tram ShedGary VinesNo ratings yet
- ANFIS Based IMC PID Controller For Permanent Magnet DC MotorDocument8 pagesANFIS Based IMC PID Controller For Permanent Magnet DC MotorAchairformy SkincareNo ratings yet
- Case Studies..... EditedDocument11 pagesCase Studies..... EditedMaina PeterNo ratings yet
- Erm Medical AbbreviationDocument1 pageErm Medical AbbreviationMehan NackeeranNo ratings yet
- Struktur Sel ProkariotDocument101 pagesStruktur Sel ProkariotRizkalNo ratings yet
- English & Maths For 3rd StandardDocument8 pagesEnglish & Maths For 3rd StandardsastryNo ratings yet
- Iahr Aiih International Symposium On Hydraulic Structures Ciudad Guayana, Venezuela, October 2006Document10 pagesIahr Aiih International Symposium On Hydraulic Structures Ciudad Guayana, Venezuela, October 2006Percy Rojas ChavezNo ratings yet
- Gwec - Global Wind Report 2024Document168 pagesGwec - Global Wind Report 2024P MandalNo ratings yet
- DevSecOpsGuides DevSecOpsGuides Com 1684505577Document297 pagesDevSecOpsGuides DevSecOpsGuides Com 1684505577KaranNo ratings yet
- Buildings For EducationDocument327 pagesBuildings For EducationEngEzequiel100% (2)
- 4TNE98-TBZ Javier MuñozDocument35 pages4TNE98-TBZ Javier Muñozjavier muñozNo ratings yet
- Parts of An Email: Business Email Writing Cheat SheetDocument14 pagesParts of An Email: Business Email Writing Cheat Sheetluluzera100% (1)
- Defense Laboratories and Centers: AFRL: Air Force Research LaboratoryDocument2 pagesDefense Laboratories and Centers: AFRL: Air Force Research LaboratoryIan S Ryu100% (1)
- Cereal CropsDocument34 pagesCereal CropsJe-ar ColipanoNo ratings yet
- Educational Leadership Management - Exam - July 2017Document1 pageEducational Leadership Management - Exam - July 2017Mazuba MutintaNo ratings yet
- Apa 7TH Edition Format ExampleDocument11 pagesApa 7TH Edition Format ExampleCory StephensonNo ratings yet
- Air Pollution: Evs Project-Class XiiDocument12 pagesAir Pollution: Evs Project-Class XiirijuNo ratings yet
- Computer Security MCQDocument12 pagesComputer Security MCQpinkudon089No ratings yet
- Open Ended Lab For Soil MechanicsDocument27 pagesOpen Ended Lab For Soil Mechanicsعثمان محيب احمدNo ratings yet
- Software VerificationDocument28 pagesSoftware VerificationAhmi khanNo ratings yet
- Bexitrol F Dpi PDFDocument4 pagesBexitrol F Dpi PDFTahia Rahman JuhiNo ratings yet
- Madison County Inspection ReportsDocument5 pagesMadison County Inspection ReportsMike BrownNo ratings yet
- Annual Report PDFDocument252 pagesAnnual Report PDFAnonymous TPVfFif6TONo ratings yet
- Current Event Lesson PlanDocument3 pagesCurrent Event Lesson Planapi-550211632No ratings yet
- Course Material Required For Board Exams 2018Document6 pagesCourse Material Required For Board Exams 2018Anh Phúc LêNo ratings yet
- Field Study 1 Chapter 3 Pandemic EditionDocument46 pagesField Study 1 Chapter 3 Pandemic EditionShaenna AliNo ratings yet