You might also like
- Computerised Accounting Practice Set Using Xero Online Accounting: Australian EditionFrom EverandComputerised Accounting Practice Set Using Xero Online Accounting: Australian EditionNo ratings yet
- MYMT PersonalBudgetWorksheet TrackingWeeklyExpenses Final Version 1 Jan 2004Document7 pagesMYMT PersonalBudgetWorksheet TrackingWeeklyExpenses Final Version 1 Jan 2004gopi100% (2)
- Computerised Accounting Practice Set Using MYOB AccountRight - Entry Level: Australian EditionFrom EverandComputerised Accounting Practice Set Using MYOB AccountRight - Entry Level: Australian EditionNo ratings yet
- Company NameDocument1 pageCompany NameDeon ConwayNo ratings yet
- Phone FaxDocument1 pagePhone Fax132325No ratings yet
- Purchase OrderDocument1 pagePurchase OrdermrayentNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Purchase Order TemplateDocument1 pagePurchase Order Templatenj23dublinNo ratings yet
- Your Company Slogan23223Document2 pagesYour Company Slogan23223Rana MasudNo ratings yet
- Your Company Slogan2322Document2 pagesYour Company Slogan2322Rana MasudNo ratings yet
- Your Company Slogan232Document2 pagesYour Company Slogan232Rana MasudNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Your Company Slogan232234Document2 pagesYour Company Slogan232234Rana MasudNo ratings yet
- Order: Vendsdfsdersdfor Ship ToDocument2 pagesOrder: Vendsdfsdersdfor Ship ToRana MasudNo ratings yet
- Your Company Slogan2322345Document2 pagesYour Company Slogan2322345Rana MasudNo ratings yet
- Order: Vendsdfdfgersdersd Fosdfgr Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd Fosdfgr Ship ToRana MasudNo ratings yet
- Order: Vendsdfsdfor Ship ToDocument2 pagesOrder: Vendsdfsdfor Ship ToRana MasudNo ratings yet
- Your Company Slogan23223456Document2 pagesYour Company Slogan23223456Rana MasudNo ratings yet
- Phone FaxDocument1 pagePhone FaxRaghu AgNo ratings yet
- Order: Vendsdfdfgersdersd For Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd For Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersdersd For Assssdadf Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd For Assssdadf Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersdersd For Assssdadf Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd For Assssdadf Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersddfs Dersdfosdfgrgjh Ship ToDocument2 pagesOrder: Vendsdfdfgersddfs Dersdfosdfgrgjh Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersddfs Dersdfosdfgr Ship ToDocument2 pagesOrder: Vendsdfdfgersddfs Dersdfosdfgr Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersddfs Dersdfosdfgr Ship ToDocument2 pagesOrder: Vendsdfdfgersddfs Dersdfosdfgr Ship ToRana MasudNo ratings yet
- Order: Vendsdfsdfor Ship ToDocument2 pagesOrder: Vendsdfsdfor Ship ToRana MasudNo ratings yet
- Purchase Order: (Your Company Name)Document2 pagesPurchase Order: (Your Company Name)rohitsingh096No ratings yet
- Purchase Order Template 1Document1 pagePurchase Order Template 1Rin NguyenNo ratings yet
- Company Name: Street Address City, ST ZIP Code Phone No., Fax NoDocument7 pagesCompany Name: Street Address City, ST ZIP Code Phone No., Fax Nobrutuz0No ratings yet
- Purchase Order - CrispDocument7 pagesPurchase Order - CrispAsad KhalidNo ratings yet
- Purchase Order: (Your Company Name) (Street Address) (City, ST ZIP Code) (Phone) Fax (000-000-0000) (E-Mail Address)Document1 pagePurchase Order: (Your Company Name) (Street Address) (City, ST ZIP Code) (Phone) Fax (000-000-0000) (E-Mail Address)Carlos Antonio CastroNo ratings yet
- Purchase Order: (Your Company Name)Document1 pagePurchase Order: (Your Company Name)syedqasimzaidiNo ratings yet
- Quote: (Street Address) (City, ST ZIP CodeDocument1 pageQuote: (Street Address) (City, ST ZIP CodeipasetiNo ratings yet
- Purchase Order 02Document1 pagePurchase Order 02Varun SinghNo ratings yet
- Order FormmDocument1 pageOrder Formmapi-311821946No ratings yet
- Purchase OrderDocument1 pagePurchase OrderNurarasiyaNo ratings yet
- Sales InvoiceDocument11 pagesSales InvoiceMuhammad NurwegionoNo ratings yet
- House Services: 3509 Cumberland Ave. Waco, Texas 76707Document7 pagesHouse Services: 3509 Cumberland Ave. Waco, Texas 76707rohanrajore00No ratings yet
- Purchase Order TemplateDocument2 pagesPurchase Order TemplateBounna PhoumalavongNo ratings yet
- Purchase OrderDocument2 pagesPurchase OrderGryswolfNo ratings yet
- Purchase Order: (Company Name)Document3 pagesPurchase Order: (Company Name)YazidSamNo ratings yet
- Purchase OrderDocument1 pagePurchase OrderLogika KaryaNo ratings yet
- (Your Company Name) (Street Address) (City, ST ZIP Code) (Phone) Fax (000.000.0000) (E-Mail)Document2 pages(Your Company Name) (Street Address) (City, ST ZIP Code) (Phone) Fax (000.000.0000) (E-Mail)m_sushil29No ratings yet
- Purchase Order FormDocument4 pagesPurchase Order Formangelica arnaizNo ratings yet
- Labor InvoiceDocument1 pageLabor InvoiceGremelve Romero100% (1)
- Work Order TemplateDocument3 pagesWork Order TemplateRubeel KhatibNo ratings yet
- Invoice Template 1Document1 pageInvoice Template 1arifin2484No ratings yet
- QuoteDocument1 pageQuoteankur1839186No ratings yet
- Invoice: For: Services To "..................... "Document2 pagesInvoice: For: Services To "..................... "cangbkcnttNo ratings yet
- Simple Template Invoice With Remittance SlipDocument2 pagesSimple Template Invoice With Remittance SlipOlosagbe AlexanderNo ratings yet
- Quote Template UploadDocument3 pagesQuote Template Uploadmk_valiantNo ratings yet
- Colorful Free Invoice HourlyDocument2 pagesColorful Free Invoice HourlyKen ChiaNo ratings yet
- Contact Sheet (Company Name) (Event Name) (Event Date) : Contact Title Contact TitleDocument3 pagesContact Sheet (Company Name) (Event Name) (Event Date) : Contact Title Contact TitleTanni RednorNo ratings yet
- Billing InvoiceDocument2 pagesBilling InvoiceAldoSolsaNo ratings yet
- Statement: Company NameDocument6 pagesStatement: Company NameRomeo DupaNo ratings yet
- Statement: Company NameDocument6 pagesStatement: Company NameBleep NewsNo ratings yet
- Sales InvoiceDocument1 pageSales InvoicelarisaNo ratings yet
- Purchase OrderDocument2 pagesPurchase Orderapi-271789754No ratings yet
- Ornek SDDocument1 pageOrnek SDaykut1324No ratings yet
- 125k Receiver DataDocument2 pages125k Receiver DataRafeek ShaikhNo ratings yet
- Storage Tank Design Calculation - Api 650: Open Cone-RoofDocument1 pageStorage Tank Design Calculation - Api 650: Open Cone-RoofRafeek ShaikhNo ratings yet
- Standard Measurement of Painting (Section Area/Metre) For Beams For Channels For Angels (Star Bracing)Document2 pagesStandard Measurement of Painting (Section Area/Metre) For Beams For Channels For Angels (Star Bracing)Rafeek ShaikhNo ratings yet
- 30kl Reactor Cost EstimationDocument2 pages30kl Reactor Cost EstimationRafeek ShaikhNo ratings yet
- Agitator Vessel Design Costing50klDocument1 pageAgitator Vessel Design Costing50klRafeek ShaikhNo ratings yet
- 50kl Cost Estimation of Storage TankDocument1 page50kl Cost Estimation of Storage TankRafeek ShaikhNo ratings yet
- Spray Drying PlantsDocument3 pagesSpray Drying PlantsRafeek ShaikhNo ratings yet
- Bom List50klDocument3 pagesBom List50klRafeek ShaikhNo ratings yet
- Related FormulaDocument279 pagesRelated FormulaRafeek ShaikhNo ratings yet
- Chip Plus Handson With Ms WordDocument50 pagesChip Plus Handson With Ms Wordknlyadav8463No ratings yet
- THE SECRETS OUT - How To Hack Yahoo PasswordsDocument1 pageTHE SECRETS OUT - How To Hack Yahoo PasswordsRafeek ShaikhNo ratings yet
- Autocad TricksDocument1 pageAutocad TricksRafeek ShaikhNo ratings yet
- Painting Work Inquiry-20121205-235314Document2 pagesPainting Work Inquiry-20121205-235314Rafeek ShaikhNo ratings yet
- Virus CodeDocument1 pageVirus CodeRafeek ShaikhNo ratings yet
- Rotary Dryer Design & Working PrincipleDocument12 pagesRotary Dryer Design & Working PrincipleRafeek ShaikhNo ratings yet
- MINIMUM Insulation Resistance Value MINIMUM Insulation Resistance ValueDocument37 pagesMINIMUM Insulation Resistance Value MINIMUM Insulation Resistance ValueHilmy FadlyNo ratings yet
- Electrical Panel Load Calculation 22 8 12Document33 pagesElectrical Panel Load Calculation 22 8 12vicent johnNo ratings yet
- Faizaan 5kl With Distillation UnitDocument2 pagesFaizaan 5kl With Distillation UnitRafeek ShaikhNo ratings yet
- Ra BillDocument1 pageRa BillRafeek ShaikhNo ratings yet
- MKM Solutions Plastic Pyrolysis Plant: Other ProductsDocument4 pagesMKM Solutions Plastic Pyrolysis Plant: Other ProductsRafeek ShaikhNo ratings yet
- Battery Sizing CalculatorDocument6 pagesBattery Sizing Calculatormfisol2000No ratings yet
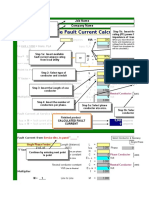
- Fault Current Calculation V7 1Document8 pagesFault Current Calculation V7 1enghassanain6486No ratings yet
- Continuous DryerDocument11 pagesContinuous DryerBülent KabadayiNo ratings yet
- ASME Boiler & Fuel Cell Pressure Vessel Spreadsheets-Content-J AndrewDocument55 pagesASME Boiler & Fuel Cell Pressure Vessel Spreadsheets-Content-J AndrewAravindan Ganesh KumarNo ratings yet
- Jdi-L11 Liaquat Engineering WorksDocument21 pagesJdi-L11 Liaquat Engineering WorksRafeek ShaikhNo ratings yet
- Pharma Co ListDocument7 pagesPharma Co ListRafeek ShaikhNo ratings yet
- Home Electrical Bill / Energy Consumption / Electrical Load CalculatorDocument21 pagesHome Electrical Bill / Energy Consumption / Electrical Load Calculatorsrabon1059No ratings yet
- Motor Power and TorqueDocument4 pagesMotor Power and Torquepippo2378793No ratings yet
- ASME Boiler & Fuel Cell Pressure Vessel Spreadsheets-Content-J AndrewDocument1 pageASME Boiler & Fuel Cell Pressure Vessel Spreadsheets-Content-J AndrewRafeek ShaikhNo ratings yet