You might also like
- Computerised Accounting Practice Set Using MYOB AccountRight - Entry Level: Australian EditionFrom EverandComputerised Accounting Practice Set Using MYOB AccountRight - Entry Level: Australian EditionNo ratings yet
- Computerised Accounting Practice Set Using Xero Online Accounting: Australian EditionFrom EverandComputerised Accounting Practice Set Using Xero Online Accounting: Australian EditionNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Purchase Order PO#100 for ABC123Document2 pagesPurchase Order PO#100 for ABC123Rana MasudNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Purchase OrderDocument1 pagePurchase OrdermrayentNo ratings yet
- Purchase Order: Vendor Ship ToDocument2 pagesPurchase Order: Vendor Ship ToRana MasudNo ratings yet
- Purchase OrderDocument1 pagePurchase OrderNurarasiyaNo ratings yet
- Your Company Slogan232Document2 pagesYour Company Slogan232Rana MasudNo ratings yet
- Your Company Slogan23223Document2 pagesYour Company Slogan23223Rana MasudNo ratings yet
- Your Company Slogan2322Document2 pagesYour Company Slogan2322Rana MasudNo ratings yet
- Purchase order for ABC123Document2 pagesPurchase order for ABC123Rana MasudNo ratings yet
- Purchase Order DetailsDocument2 pagesPurchase Order Detailsrohitsingh096No ratings yet
- Order for ABC123 from Company NameDocument2 pagesOrder for ABC123 from Company NameRana MasudNo ratings yet
- Order: Vendsdfsdersdfor Ship ToDocument2 pagesOrder: Vendsdfsdersdfor Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersdersd Fosdfgr Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd Fosdfgr Ship ToRana MasudNo ratings yet
- Order: Vendsdfsdfor Ship ToDocument2 pagesOrder: Vendsdfsdfor Ship ToRana MasudNo ratings yet
- Order summary for ABC123Document2 pagesOrder summary for ABC123Rana MasudNo ratings yet
- Order summary for ABC123Document2 pagesOrder summary for ABC123Rana MasudNo ratings yet
- Your Company Slogan2322345Document2 pagesYour Company Slogan2322345Rana MasudNo ratings yet
- Order: Vendsdfdfgersddfs Dersdfosdfgrgjh Ship ToDocument2 pagesOrder: Vendsdfdfgersddfs Dersdfosdfgrgjh Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersdersd For Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd For Ship ToRana MasudNo ratings yet
- Your Company Slogan23223456Document2 pagesYour Company Slogan23223456Rana MasudNo ratings yet
- Order: Vendsdfdfgersdersd For Assssdadf Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd For Assssdadf Ship ToRana MasudNo ratings yet
- Order: Vendsdfdfgersdersd For Assssdadf Ship ToDocument2 pagesOrder: Vendsdfdfgersdersd For Assssdadf Ship ToRana MasudNo ratings yet
- Purchase Order Template for Company NameDocument1 pagePurchase Order Template for Company NameCarlos Antonio CastroNo ratings yet
- Purchase Order for Company NameDocument1 pagePurchase Order for Company Namenj23dublinNo ratings yet
- (Your Company Name) (Street Address) (City, ST ZIP Code) (Phone) Fax (000.000.0000) (E-Mail)Document2 pages(Your Company Name) (Street Address) (City, ST ZIP Code) (Phone) Fax (000.000.0000) (E-Mail)m_sushil29No ratings yet
- Purchase Order: (Your Company Name)Document2 pagesPurchase Order: (Your Company Name)Edy RiadiNo ratings yet
- Work Order 1Document1 pageWork Order 1Rafeek ShaikhNo ratings yet
- Purchase OrderDocument1 pagePurchase OrderLogika KaryaNo ratings yet
- Company NameDocument1 pageCompany NameDeon ConwayNo ratings yet
- Invoice: For: Services To "..................... "Document2 pagesInvoice: For: Services To "..................... "cangbkcnttNo ratings yet
- Purchase Order Template 1Document1 pagePurchase Order Template 1Rin NguyenNo ratings yet
- Phone FaxDocument1 pagePhone Fax132325No ratings yet
- Company Name: Street Address City, ST ZIP Code Phone No., Fax NoDocument7 pagesCompany Name: Street Address City, ST ZIP Code Phone No., Fax Nobrutuz0No ratings yet
- Quotation BPHDocument1 pageQuotation BPHHasbullah Mohamad SalihNo ratings yet
- Purchase Order - CrispDocument7 pagesPurchase Order - CrispAsad KhalidNo ratings yet
- Quote: (Street Address) (City, ST ZIP CodeDocument1 pageQuote: (Street Address) (City, ST ZIP CodeipasetiNo ratings yet
- Blank Purchase Order FormDocument2 pagesBlank Purchase Order FormSyah EarulNo ratings yet
- QuoteDocument1 pageQuoteankur1839186No ratings yet
- Sales InvoiceDocument11 pagesSales InvoiceMuhammad NurwegionoNo ratings yet
- Invoice Template with Service Fee and Labor ChargesDocument2 pagesInvoice Template with Service Fee and Labor ChargesAldoSolsaNo ratings yet
- Purchase OrderDocument1 pagePurchase OrderikramwzNo ratings yet
- Invoice for ABC12345 with job due date and sales detailsDocument1 pageInvoice for ABC12345 with job due date and sales detailsarifin2484No ratings yet
- Purchase Order Summary for CompanyDocument1 pagePurchase Order Summary for CompanyVarun SinghNo ratings yet
- Document 3Document1 pageDocument 3elenaNo ratings yet
- Purchase OrderDocument1 pagePurchase OrderShava KairaNo ratings yet
- Invoice SampleDocument1 pageInvoice Sampleolgutza123No ratings yet
- 06 Sales-InvoiceDocument4 pages06 Sales-InvoicehfjfjfjNo ratings yet
- Sales Quote for Services and PartsDocument3 pagesSales Quote for Services and Partsmk_valiantNo ratings yet
- Packing Slip TemplateDocument5 pagesPacking Slip TemplateLuzNo ratings yet
- Contoh Nota Penjualan Dengan Desain Yang SimpelDocument1 pageContoh Nota Penjualan Dengan Desain Yang SimpelNah GiniNo ratings yet
- Complaint LetterDocument1 pageComplaint LetterkktuaNo ratings yet
- Purchase Order: (Company Name)Document3 pagesPurchase Order: (Company Name)YazidSamNo ratings yet
- Car Sales TestDocument4 pagesCar Sales Testcarbajal1980No ratings yet
- Sales Quotation Template For ExcelDocument2 pagesSales Quotation Template For ExcelsaadNo ratings yet
- Order FormDocument1 pageOrder FormNik Ahmad HafizuddinNo ratings yet
- Purchase OrderDocument2 pagesPurchase Orderapi-271789754No ratings yet
- Service-InvoiceDocument3 pagesService-InvoiceAvcipsids JCthh IdsNo ratings yet
- PTD - Travel Agencies Act 1976Document12 pagesPTD - Travel Agencies Act 1976syedqasimzaidiNo ratings yet
- Compact Zoom Lens Comparison Chart for 4K ProductionDocument2 pagesCompact Zoom Lens Comparison Chart for 4K ProductionfreebooksNo ratings yet
- Wedding Guest ListDocument1 pageWedding Guest ListsyedqasimzaidiNo ratings yet
- Repeated PPRA text documentDocument104 pagesRepeated PPRA text documentImran MukhtarNo ratings yet
- Consumer Laws in PakistanDocument95 pagesConsumer Laws in PakistanSindh001No ratings yet
- Yearly CalendarDocument1 pageYearly CalendarsyedqasimzaidiNo ratings yet
- Toyota Passo Panel DiscriptionDocument1 pageToyota Passo Panel DiscriptionsyedqasimzaidiNo ratings yet
- MC Sampler Pack PDFDocument195 pagesMC Sampler Pack PDFVedaste Ndayishimiye100% (2)
- Tjv13n1chinese LambDocument11 pagesTjv13n1chinese LambDennyHalim.comNo ratings yet
- Art'S A Waste of Time ! Just Forget About It !: Arco Wants To Study Music, But His Parents Are Against The IdeaDocument12 pagesArt'S A Waste of Time ! Just Forget About It !: Arco Wants To Study Music, But His Parents Are Against The IdeaTzar UmangNo ratings yet
- Excel Formulas A Quick List PDFDocument6 pagesExcel Formulas A Quick List PDFIrfan Abbasi100% (1)
- Weekly PlannerDocument1 pageWeekly PlannersyedqasimzaidiNo ratings yet
- Rent Receipt: One Thousand Two Hundred Thirty-Four and 56/100 DollarsDocument1 pageRent Receipt: One Thousand Two Hundred Thirty-Four and 56/100 DollarssyedqasimzaidiNo ratings yet
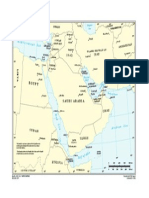
- Middle East InfoDocument1 pageMiddle East InfosyedqasimzaidiNo ratings yet
- FaqDocument5 pagesFaqsyedqasimzaidiNo ratings yet
- MC Sampler Pack PDFDocument195 pagesMC Sampler Pack PDFVedaste Ndayishimiye100% (2)
- Early KoreanDocument4 pagesEarly KoreansyedqasimzaidiNo ratings yet
- Kids' foot sizing chart find widths sizesDocument1 pageKids' foot sizing chart find widths sizesdeibendeileNo ratings yet
- Po EunDocument2 pagesPo EunsyedqasimzaidiNo ratings yet
- Immuniation Schedule Hs 472Document2 pagesImmuniation Schedule Hs 472api-272755914No ratings yet
- Kids' foot sizing chart find widths sizesDocument1 pageKids' foot sizing chart find widths sizesdeibendeileNo ratings yet
- Downs 3Document5 pagesDowns 3Diaz Hazrina SetiadiNo ratings yet
- A Pocket Guide To Blood Pressure Measurement in ChildrenDocument4 pagesA Pocket Guide To Blood Pressure Measurement in ChildrenKira23406No ratings yet
- Math Standards PDFDocument93 pagesMath Standards PDFjason1989No ratings yet
- Child Development ChartDocument1 pageChild Development ChartDevelopmentChart100% (4)
- 0 - 18yrs Schedule of VaccineDocument4 pages0 - 18yrs Schedule of VaccineEmanGamalAlbazNo ratings yet
- Advanced CalculusDocument592 pagesAdvanced Calculusjosemarcelod7088No ratings yet
- Chart Pattern ABCD-BullishDocument2 pagesChart Pattern ABCD-BullishsyedqasimzaidiNo ratings yet
- Fund ChartDocument9 pagesFund ChartsyedqasimzaidiNo ratings yet