You might also like
- Medical Surgical NursingDocument146 pagesMedical Surgical Nursingnisha jomonNo ratings yet
- Coronary Calcium ScoreDocument49 pagesCoronary Calcium ScoreBinod KumarNo ratings yet
- Pathology of Cardiovascular SystemDocument75 pagesPathology of Cardiovascular Systemefri100% (2)
- MRCP AnswersDocument139 pagesMRCP Answerspal_pal_palNo ratings yet
- Awareness Under AnesthesiaDocument27 pagesAwareness Under AnesthesiaagatakassaNo ratings yet
- Failed Spinal AnaesthesiaDocument10 pagesFailed Spinal Anaesthesian12345678n100% (1)
- Anaesthetic Management of Joint Replacement SurgeriesDocument55 pagesAnaesthetic Management of Joint Replacement SurgeriesRaguNo ratings yet
- Elsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFDocument230 pagesElsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFMila KarmilaNo ratings yet
- Management of Acute PainDocument76 pagesManagement of Acute PainAnonymous nruHyuwtJ100% (1)
- Abbott Istat PDFDocument4 pagesAbbott Istat PDFMedLab Professional100% (1)
- Anesthesia in High Risk Patients PDFDocument341 pagesAnesthesia in High Risk Patients PDFpopoying100% (4)
- Amboss ECGDocument13 pagesAmboss ECGAllysahNo ratings yet
- Paediatric Anaesthesia PDFDocument33 pagesPaediatric Anaesthesia PDFMarcelitaTaliaDuwiriNo ratings yet
- CPG Management of Atrial Fibrillation PDFDocument119 pagesCPG Management of Atrial Fibrillation PDFZee YongNo ratings yet
- @anesthesia Books 2018 GuidelinesDocument16 pages@anesthesia Books 2018 GuidelinesAgil Rumboko SumitroNo ratings yet
- Anaesthesia Record KeepingDocument48 pagesAnaesthesia Record Keepingrahmaya100% (1)
- Pharmacotherapeutics - PharmD II YearDocument5 pagesPharmacotherapeutics - PharmD II YearSuresh Thanneru100% (2)
- Sample Write UpDocument4 pagesSample Write UpMaha Mohamed100% (1)
- AA Course-Difficult Airway1Document54 pagesAA Course-Difficult Airway1Anonymous V5xDcrNo ratings yet
- Asa 2013Document1,076 pagesAsa 2013Marwa Mahrous100% (4)
- Color Code AnesthesiaDocument6 pagesColor Code AnesthesiaYusnia Gulfa MaharaniNo ratings yet
- St. Joseph'S High School San Narciso, QuezonDocument22 pagesSt. Joseph'S High School San Narciso, QuezonDaphane Kate AureadaNo ratings yet
- Airway Management Inside and Outside Operating Rooms 2018 British Journal ofDocument3 pagesAirway Management Inside and Outside Operating Rooms 2018 British Journal ofSeveNNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Perioperative ManagementDocument3 pagesPerioperative ManagementRaymond De GulaNo ratings yet
- Primary Care Referral Guidelines 13.04.2014compile Version - MasturaDocument8 pagesPrimary Care Referral Guidelines 13.04.2014compile Version - Masturaamalina roshimi0% (4)
- @anesthesia Books 2017 HandbookDocument835 pages@anesthesia Books 2017 Handbookmichele.funatoNo ratings yet
- FCA 2 Trials MindmapDocument1 pageFCA 2 Trials MindmapameenallyNo ratings yet
- @anesthesia Books 2018 Neuroanesthesia Crisis Manual DepartmentDocument56 pages@anesthesia Books 2018 Neuroanesthesia Crisis Manual DepartmentLizzeth Inés Sánchez MendozaNo ratings yet
- Medical Aspects of Fitness For Offshore Work PDFDocument22 pagesMedical Aspects of Fitness For Offshore Work PDFParth DM100% (1)
- OSA and Periop Complications 2012Document9 pagesOSA and Periop Complications 2012cjbae22No ratings yet
- Neuraxial Anesthesia - Analgesia Techniques in The Patient Receiving Anticoagulant or Antiplatelet Medication - UpToDateDocument25 pagesNeuraxial Anesthesia - Analgesia Techniques in The Patient Receiving Anticoagulant or Antiplatelet Medication - UpToDatemago1961100% (1)
- Oet Materials 2Document201 pagesOet Materials 2jojan100% (4)
- Anesthesia For The Patient With Peripartum Hemorrhage - UpToDateDocument25 pagesAnesthesia For The Patient With Peripartum Hemorrhage - UpToDateZurya UdayanaNo ratings yet
- Extubation After AnaesthesiaDocument7 pagesExtubation After AnaesthesiaaksinuNo ratings yet
- Eras Bps Final Nov2017 2Document24 pagesEras Bps Final Nov2017 2Wardah Fauziah El SofwanNo ratings yet
- 2022 Preoperative Assessment Premedication Perioperative DocumentationDocument38 pages2022 Preoperative Assessment Premedication Perioperative DocumentationMohmmed Mousa100% (1)
- Anesthesia For Patients With Renal DiseaseDocument4 pagesAnesthesia For Patients With Renal DiseasejoninhabNo ratings yet
- April 2021 - Pediatric Emergency CareDocument128 pagesApril 2021 - Pediatric Emergency CareEdison Junior Juarez LaricoNo ratings yet
- Safe Sedation Practice For Healthcare Procedures: Standards and GuidanceDocument39 pagesSafe Sedation Practice For Healthcare Procedures: Standards and GuidanceAlaa ShnienNo ratings yet
- Who Guidelines For Safe SurgeryDocument173 pagesWho Guidelines For Safe SurgeryAhmed M Frieg100% (1)
- Postpartum Hemorrhage With A Standardized Massive Transfusion ProtocolDocument9 pagesPostpartum Hemorrhage With A Standardized Massive Transfusion Protocolmedicinaun74100% (2)
- Millers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Document44 pagesMillers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Adriana VickNo ratings yet
- Monitored Anesthesia Care in Adults: Considerations During Covid-19 PandemicDocument29 pagesMonitored Anesthesia Care in Adults: Considerations During Covid-19 PandemicGanda Impola TBANo ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- 4 5821337585678549749 PDFDocument75 pages4 5821337585678549749 PDFardesh abdilleNo ratings yet
- Recommendations For Standards of Monitoring During Anaesthesia and Recovery 2021Document14 pagesRecommendations For Standards of Monitoring During Anaesthesia and Recovery 2021Ahmad Fairuz Abdul ShokriNo ratings yet
- 1.05 (Surgery) General Anesthesia - Airway ManagementDocument3 pages1.05 (Surgery) General Anesthesia - Airway ManagementLeo Mari Go LimNo ratings yet
- Day Case For WebDocument34 pagesDay Case For WebDavid CruzNo ratings yet
- Immediate Post Anesthetic RecoveryDocument12 pagesImmediate Post Anesthetic Recoverysubvig100% (2)
- Preoxygenation During Induction of Anesthesia in Noncritically Ill PatientsDocument6 pagesPreoxygenation During Induction of Anesthesia in Noncritically Ill PatientsasfwegereNo ratings yet
- Vaishali Syal Moderator - Prof. J. R. ThakurDocument34 pagesVaishali Syal Moderator - Prof. J. R. ThakurTasha NurfitrianiNo ratings yet
- SAJAA (V27) p11-16 2726 FCA SupplementDocument5 pagesSAJAA (V27) p11-16 2726 FCA SupplementCarolina SartiniNo ratings yet
- FCA (SA) Portfolio 7-5-2013Document39 pagesFCA (SA) Portfolio 7-5-2013matentenNo ratings yet
- Airway Pharmacology: Anesthesia KeyDocument19 pagesAirway Pharmacology: Anesthesia KeyChrispin FaithNo ratings yet
- Practice Guidelines For Juniors 01 June 2016Document3 pagesPractice Guidelines For Juniors 01 June 2016ElaineNo ratings yet
- Effect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyDocument10 pagesEffect of Magnesium Sulphate On Intraoperative Hemodynamic Responses in Laparoscopic CholecystectomyIOSRjournalNo ratings yet
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDocument14 pagesOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhNo ratings yet
- Pediatric Regional Anesthesia 2005Document66 pagesPediatric Regional Anesthesia 2005tameem89No ratings yet
- Principles of Balanced AnesthesiaDocument2 pagesPrinciples of Balanced AnesthesiaZahra ZakiyyahNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
- Manejo de Las Crisis en Anestesia - Gaba 2 Ed PDFDocument424 pagesManejo de Las Crisis en Anestesia - Gaba 2 Ed PDFdianisssuxNo ratings yet
- Example of RCA Medication ErrorDocument5 pagesExample of RCA Medication ErrorAnonymous CjzFZgt50% (2)
- N E D L G National Essential Drug List &guidelinesDocument32 pagesN E D L G National Essential Drug List &guidelinesportosinNo ratings yet
- Operational Guidelines For Clients' Rights and Providers' Rights-DutiesDocument34 pagesOperational Guidelines For Clients' Rights and Providers' Rights-DutiesVichhai100% (1)
- Anesthesia TechnicianDocument1 pageAnesthesia TechnicianmahbbobNo ratings yet
- To Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesDocument4 pagesTo Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 029 Reddy PDFDocument59 pages029 Reddy PDFKonas Xi PalembangNo ratings yet
- Standard Drug Concentrations and Smart-Pump Technology Reduce Continuous Medication Infusion Errors in Pediatric PatientsDocument7 pagesStandard Drug Concentrations and Smart-Pump Technology Reduce Continuous Medication Infusion Errors in Pediatric PatientsfatimamalmeidaNo ratings yet
- Perioperative Management of Patients Receiving Anticoagulants - UpToDateDocument65 pagesPerioperative Management of Patients Receiving Anticoagulants - UpToDatejames lxNo ratings yet
- Case StudyDocument32 pagesCase Studyapi-407110554No ratings yet
- Waiting As Remedy - The Architecture of Emergent CareDocument34 pagesWaiting As Remedy - The Architecture of Emergent CareJoey GaoNo ratings yet
- Test - Surgery Book MCQs - Final Exam - QuizletDocument158 pagesTest - Surgery Book MCQs - Final Exam - Quizlety SNo ratings yet
- 2021 Article 605Document17 pages2021 Article 605Flor VelasquezNo ratings yet
- HUKM PharmacyDocument2 pagesHUKM PharmacyLua Chiyar LockNo ratings yet
- Call To See Patient PDFDocument111 pagesCall To See Patient PDFKevin KhawNo ratings yet
- Red Cross Als Prep Packet 2020Document69 pagesRed Cross Als Prep Packet 2020asdkjNo ratings yet
- University of The Philippines ManilaDocument11 pagesUniversity of The Philippines ManilaAngeli Jean Koreen CorpuzNo ratings yet
- What Is Heart Bypass SurgeryDocument10 pagesWhat Is Heart Bypass SurgeryVanitha AlagarsamyNo ratings yet
- The Influence of Gong Waning Music Therapy Toward Anxiety in Patients With Acute Coronary SyndromeDocument16 pagesThe Influence of Gong Waning Music Therapy Toward Anxiety in Patients With Acute Coronary SyndromeErna sariNo ratings yet
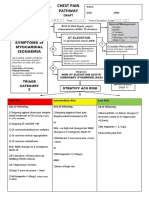
- Chest Pain Pathway May 2014Document4 pagesChest Pain Pathway May 2014fauzanNo ratings yet
- ANNEX F Employees History and Physical Exam Form 1 - 240205 - 092840Document6 pagesANNEX F Employees History and Physical Exam Form 1 - 240205 - 092840Marion Pierre MateoNo ratings yet
- Duration of Dual Antiplatelet Therapy: Current ControversiesDocument8 pagesDuration of Dual Antiplatelet Therapy: Current ControversiesRajendra ChavanNo ratings yet
- Concept MapDocument4 pagesConcept Mapdejosep_informaticsNo ratings yet
- Efficacy of Nicotine in Preventing COVID-19 Infection - Full Text View - ClinicalTrials - GovDocument8 pagesEfficacy of Nicotine in Preventing COVID-19 Infection - Full Text View - ClinicalTrials - GovRajudibNo ratings yet
- MEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncDocument14 pagesMEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncIrma DamayantiNo ratings yet