You might also like
- Science Learner Module-130708064905-Php Appilcation01 :)Document350 pagesScience Learner Module-130708064905-Php Appilcation01 :)William Bryle Pertos75% (4)
- Teacher's ProfileDocument1 pageTeacher's ProfileShim CharenNo ratings yet
- Life Camp Registration FormDocument2 pagesLife Camp Registration Formlife_campNo ratings yet
- Women's Education Academy Admission FormDocument2 pagesWomen's Education Academy Admission FormmzeqtaNo ratings yet
- CFWP Profile FormDocument1 pageCFWP Profile FormMaja Aira BumatayNo ratings yet
- 2016 DCI Internship ApplicationDocument2 pages2016 DCI Internship ApplicationSami EronNo ratings yet
- Register for Youth Mock Parliament at MSUDocument1 pageRegister for Youth Mock Parliament at MSUbrahmbhattkhushNo ratings yet
- ANNEX B_ CFWP PROFILE FORMDocument1 pageANNEX B_ CFWP PROFILE FORMjunrayguanunezNo ratings yet
- VVC Child Development Membership FormDocument1 pageVVC Child Development Membership Formcynthia19gNo ratings yet
- Canossa College Student Profile Form 2016-2017Document1 pageCanossa College Student Profile Form 2016-2017Grace BicoNo ratings yet
- Water Wars - RegistrationDocument1 pageWater Wars - RegistrationJessicaYahnertMasserNo ratings yet
- Workshop RegistrationDocument1 pageWorkshop Registrationapi-295766279No ratings yet
- Membership FormDocument1 pageMembership FormDexie EscoNo ratings yet
- PDS - Fe Marie SusubanDocument1 pagePDS - Fe Marie SusubanVanessa May Caseres GaNo ratings yet
- LIFE Registration Form 2011Document1 pageLIFE Registration Form 2011life_campNo ratings yet
- S L ApplicationDocument1 pageS L Applicationapi-239684758No ratings yet
- Registration Form 2020Document1 pageRegistration Form 2020api-366535357No ratings yet
- Biodata Template PhilippinesDocument2 pagesBiodata Template Philippinesana mae estaresNo ratings yet
- Childs Information USDocument1 pageChilds Information USashishgaur007No ratings yet
- Sugbusog Sa Eskuylahan Entry Form: Division Focal PersonDocument1 pageSugbusog Sa Eskuylahan Entry Form: Division Focal PersonMarlyn Caballero100% (1)
- Parental ConsentDocument1 pageParental ConsentJennette BelliotNo ratings yet
- Campus Ministry Choir Audition FormDocument1 pageCampus Ministry Choir Audition FormFern HofileñaNo ratings yet
- High School Scholarship Application DeadlineDocument3 pagesHigh School Scholarship Application DeadlineAndri ImanudinNo ratings yet
- UPLB College Forestry ApplicationDocument2 pagesUPLB College Forestry ApplicationdamcelletNo ratings yet
- Leave LetterDocument1 pageLeave LetterKilaine MontillaNo ratings yet
- Summer 2014 Registration FormDocument1 pageSummer 2014 Registration Formapi-252184858No ratings yet
- MSL Member InfoDocument2 pagesMSL Member InfomeridianstreamlinersNo ratings yet
- KHQA WeatherWizForm 2019Document1 pageKHQA WeatherWizForm 2019KHQA News100% (1)
- Individual Inventory FormDocument1 pageIndividual Inventory FormMona Liza ZurawNo ratings yet
- Application For Admission BedDocument3 pagesApplication For Admission Bedcasna lhorNo ratings yet
- New Student Information Sheet: Code IDDocument1 pageNew Student Information Sheet: Code IDUmamaAhmedNo ratings yet
- Bumi Resources Internship Application FormDocument1 pageBumi Resources Internship Application FormNey0No ratings yet
- Staff ApplicationDocument3 pagesStaff ApplicationJordan HerringNo ratings yet
- Personal Information:: Paste Your Recent Passport Size PhotographDocument4 pagesPersonal Information:: Paste Your Recent Passport Size PhotographkuberkNo ratings yet
- Bison Scholars Nomination FormDocument1 pageBison Scholars Nomination FormmortensenkNo ratings yet
- Annex e - Counselee's DataDocument2 pagesAnnex e - Counselee's DataMILEN GONZALNo ratings yet
- SSC Admision Form 2021 2022Document1 pageSSC Admision Form 2021 2022Duedate AgapitoNo ratings yet
- Sunday School Registration 2014-15Document1 pageSunday School Registration 2014-15api-249234590No ratings yet
- Student Application Form: Ects - European Credit Transfer and Accumulation SystemDocument3 pagesStudent Application Form: Ects - European Credit Transfer and Accumulation SystemMichael DoerflerNo ratings yet
- resume-3Document1 pageresume-3samueldomalaon1970No ratings yet
- Waskowitz Environmental Leadership & ServiceDocument3 pagesWaskowitz Environmental Leadership & Servicevirginia.philbrookNo ratings yet
- Supplementary Information Sheet (1) - 2Document1 pageSupplementary Information Sheet (1) - 2Jayrone James FuerteNo ratings yet
- 2011 Chocolate Championships RegistrationDocument1 page2011 Chocolate Championships RegistrationMELYONSTKDNo ratings yet
- Lindenwood University School of Education Internship Placement FormDocument3 pagesLindenwood University School of Education Internship Placement Formvictoryd5No ratings yet
- Registration FormDocument2 pagesRegistration FormMarco Villadelrey EnriquezNo ratings yet
- Bahria University Application FormDocument1 pageBahria University Application FormSarwan AliNo ratings yet
- Faculty CV FormDocument1 pageFaculty CV FormAgha JahanzebNo ratings yet
- Faculty-CV-Form JasfhsbfkDocument1 pageFaculty-CV-Form JasfhsbfkSani1248No ratings yet
- Bahria University Application FormDocument1 pageBahria University Application FormAnonymous 4uMO0p26omNo ratings yet
- Faculty CV FormDocument1 pageFaculty CV FormSani1248No ratings yet
- Sugbusog Entry Form Round 3 2023Document1 pageSugbusog Entry Form Round 3 2023Marlyn Caballero100% (2)
- Municipal Scholarship ApplicationDocument2 pagesMunicipal Scholarship ApplicationRuth BolongaitaNo ratings yet
- Yv Volunteer Application Rev1Document2 pagesYv Volunteer Application Rev1api-249338600No ratings yet
- Enrollment FormDocument1 pageEnrollment FormalliejorgensonNo ratings yet
- Cadet Information SheetDocument2 pagesCadet Information SheetVERNA GARCHITORENANo ratings yet
- Ficha Inscrição ClubeDocument1 pageFicha Inscrição ClubeisabelrabacaNo ratings yet
- INTAKE SHEET FormDocument3 pagesINTAKE SHEET FormKim MacadangdangNo ratings yet
- Tot Swimming Winter 2014Document1 pageTot Swimming Winter 2014jmfleckNo ratings yet
- 16-17 Lhs Alumni ApplicationDocument1 page16-17 Lhs Alumni Applicationapi-327409583No ratings yet
- Ojt Appeal LetterDocument2 pagesOjt Appeal LetterT.j. Peñano100% (1)
- Barrage Model.2Document1 pageBarrage Model.2T.j. PeñanoNo ratings yet
- Section A-A Rev.0Document1 pageSection A-A Rev.0T.j. PeñanoNo ratings yet
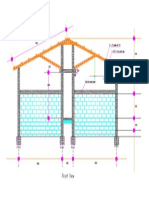
- Front ViewDocument1 pageFront ViewT.j. PeñanoNo ratings yet
- Section B-B Rev.0Document1 pageSection B-B Rev.0T.j. PeñanoNo ratings yet
- DLTC 2k14 Registration FormDocument2 pagesDLTC 2k14 Registration FormT.j. PeñanoNo ratings yet
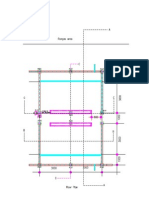
- Floor Plan Rev.0Document1 pageFloor Plan Rev.0T.j. PeñanoNo ratings yet
- Section C-C Rev.0Document1 pageSection C-C Rev.0T.j. PeñanoNo ratings yet
- Timothy Joseph Galicinao Peñano: ObjectiveDocument2 pagesTimothy Joseph Galicinao Peñano: ObjectiveT.j. PeñanoNo ratings yet
- Timothy Joseph Galicinao Peñano: ObjectiveDocument2 pagesTimothy Joseph Galicinao Peñano: ObjectiveT.j. PeñanoNo ratings yet
- Sitecom WL 183 Full ManualDocument60 pagesSitecom WL 183 Full ManualHipolito LopesNo ratings yet
- Introduction To NehemiahDocument11 pagesIntroduction To NehemiahT.j. PeñanoNo ratings yet
- Boboy CVDocument2 pagesBoboy CVT.j. PeñanoNo ratings yet
- DLTC 2k14 Interview Form For DelegatesDocument4 pagesDLTC 2k14 Interview Form For DelegatesT.j. PeñanoNo ratings yet
- Boboy CVDocument2 pagesBoboy CVT.j. PeñanoNo ratings yet
- Hello WorldDocument1 pageHello WorldT.j. PeñanoNo ratings yet