You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Maverick Men: The True Story Behind The Videos (FREE TEASER)Document25 pagesMaverick Men: The True Story Behind The Videos (FREE TEASER)Anthony DiFiore100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Essential Hypertension ManagementDocument5 pagesEssential Hypertension Managementspicychips7No ratings yet
- Movement DisordersDocument6 pagesMovement Disordersspicychips7No ratings yet
- MeningitisDocument6 pagesMeningitisspicychips7No ratings yet
- E RacerDocument17 pagesE Racerspicychips7No ratings yet
- Neuromuscular Junction Disorders: Applied AnatomyDocument6 pagesNeuromuscular Junction Disorders: Applied Anatomyspicychips7No ratings yet
- Introduction To NeurologyDocument6 pagesIntroduction To Neurologyspicychips7No ratings yet
- EncephalitisDocument4 pagesEncephalitisspicychips7No ratings yet
- Diabetes Insipidus (Di) : Etiology and ClassificationDocument6 pagesDiabetes Insipidus (Di) : Etiology and Classificationspicychips7No ratings yet
- Class StartersDocument1 pageClass Startersspicychips7No ratings yet
- Thyroid Disorders: Physiology of Thyroid HarmonesDocument68 pagesThyroid Disorders: Physiology of Thyroid Harmonesspicychips7No ratings yet
- Surgery Paper 1 Topic Frequency: Eneral UrgeryDocument3 pagesSurgery Paper 1 Topic Frequency: Eneral Urgeryspicychips7No ratings yet
- Diabetes Mellitus 1Document7 pagesDiabetes Mellitus 1spicychips7No ratings yet
- Adrenal Glands and Addison'sDocument6 pagesAdrenal Glands and Addison'sspicychips7No ratings yet
- HypoglycemiaDocument3 pagesHypoglycemiaspicychips7No ratings yet
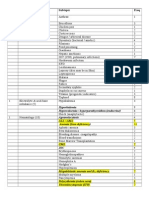
- Paper Topic (Marks) Subtopic Freq: Hyperkalemia Hypercalcemia / Hyperparathyroidism (Endocrine) Agranulocytosis All / AmlDocument5 pagesPaper Topic (Marks) Subtopic Freq: Hyperkalemia Hypercalcemia / Hyperparathyroidism (Endocrine) Agranulocytosis All / Amlspicychips7No ratings yet
- Personality Types by Eric PartakerDocument1 pagePersonality Types by Eric Partakermanishmangal2008No ratings yet
- Sonnet 54Document7 pagesSonnet 54api-272948113No ratings yet
- CS-Agricultural Drone Operation Level II-2021-03-28Document74 pagesCS-Agricultural Drone Operation Level II-2021-03-28Jessa Airam LigutomNo ratings yet
- Bus 5115 - Discussion Forum Unit 1 University of The PeopleDocument5 pagesBus 5115 - Discussion Forum Unit 1 University of The Peoplechristian allosNo ratings yet
- Blocki 2007Document5 pagesBlocki 2007Abdellah LAHDILINo ratings yet
- (PDF) Natural Language Processing With Tensorflow: Teach Language To Machines Using Python'S Deep Learning Library by Thushan GanegedaraDocument3 pages(PDF) Natural Language Processing With Tensorflow: Teach Language To Machines Using Python'S Deep Learning Library by Thushan GanegedaraBenit JajaNo ratings yet
- EDST5806 - Assessment Task 1Document10 pagesEDST5806 - Assessment Task 1vu_minh1995_60171068No ratings yet
- Artificial PassengerDocument22 pagesArtificial PassengerSiri LahariNo ratings yet
- Chapter 2 - System PlanningDocument40 pagesChapter 2 - System PlanningJia Ming100% (1)
- CMucat Application FormDocument1 pageCMucat Application FormJiyan Litohon100% (1)
- Teaching NotesDocument13 pagesTeaching NotesmaxventoNo ratings yet
- Dvar Torah FinalDocument5 pagesDvar Torah FinalKarry TaylorNo ratings yet
- DifferentiationsDocument20 pagesDifferentiationsShreyansh KashaudhanNo ratings yet
- Laws Relating To Sexual Harrassment in IndiaDocument8 pagesLaws Relating To Sexual Harrassment in IndiaAayush GondaleNo ratings yet
- Lesson Plan (1) FrogDocument4 pagesLesson Plan (1) FrogSabha HamadNo ratings yet
- DR Shamsul BaharDocument31 pagesDR Shamsul Bahardenesh11No ratings yet
- Therotical FrameworkDocument68 pagesTherotical FrameworkVipul ParekhNo ratings yet
- MEDICAL TRANSLATION INSTRUCTIONS v.1Document2 pagesMEDICAL TRANSLATION INSTRUCTIONS v.1MedinNo ratings yet
- Revilla - Nomerto Jr. M 19 4767 933Document14 pagesRevilla - Nomerto Jr. M 19 4767 933Maestro MertzNo ratings yet
- Rewards and Challenges of Being A Manager RewardsDocument22 pagesRewards and Challenges of Being A Manager Rewardsmaliha arpaNo ratings yet
- MyTradeTV Glass and Glazing Digital Magazine July 2015Document148 pagesMyTradeTV Glass and Glazing Digital Magazine July 2015Lee ClarkeNo ratings yet
- PCR Types and Its ApplicationsDocument68 pagesPCR Types and Its ApplicationsShefali Pawar100% (1)
- The Role of Language in Childrens Cognitive Development Education EssayDocument9 pagesThe Role of Language in Childrens Cognitive Development Education EssayNa shNo ratings yet
- PAPER PHYSICS (Kelompok 21 )Document4 pagesPAPER PHYSICS (Kelompok 21 )magfirahNo ratings yet
- Posh SQ L Wall ChartDocument1 pagePosh SQ L Wall Chartjoselara19No ratings yet
- Stat 132 SyllabusDocument3 pagesStat 132 SyllabusPCCPatronNo ratings yet
- Clean Edge RazorDocument14 pagesClean Edge RazorOyedele AjagbeNo ratings yet
- Sentence Completion SkillsDocument50 pagesSentence Completion SkillsJozh EusebioNo ratings yet