You might also like
- Risk RegisterDocument20 pagesRisk Registerzayzan100% (2)
- QuestionnaireDocument7 pagesQuestionnaireAnjo Pasiolco CanicosaNo ratings yet
- 1 Learning A First Language NewDocument42 pages1 Learning A First Language NewlittlefbitchNo ratings yet
- Neo Ffi 19214027Document8 pagesNeo Ffi 19214027Sehaj BediNo ratings yet
- Advanced Construction TechniquesDocument14 pagesAdvanced Construction TechniquesKristia Jolina Buendia AldeNo ratings yet
- Language AcquisitionDocument40 pagesLanguage AcquisitionLovelyn MaristelaNo ratings yet
- Movie Review, FearlessDocument6 pagesMovie Review, Fearlessmjbrennan99No ratings yet
- English Grammar and Composition: Vii STDDocument244 pagesEnglish Grammar and Composition: Vii STDAadi100% (2)
- Language DisordersDocument11 pagesLanguage DisordersAli Sahbani Harahap100% (1)
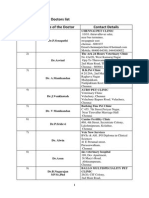
- Chennai Veterinary Doctors ListDocument7 pagesChennai Veterinary Doctors Listsrinivasa777100% (1)
- Ethics in PsychologyDocument6 pagesEthics in PsychologySafa QasimNo ratings yet
- Information Processing TheoryDocument7 pagesInformation Processing TheoryRonald GuevarraNo ratings yet
- Review of Related LiteratureDocument28 pagesReview of Related LiteratureporseenaNo ratings yet
- Pajares y Valiente 2002 Student S Self Efficacy in Their Self Regulated Learning StrategiesDocument11 pagesPajares y Valiente 2002 Student S Self Efficacy in Their Self Regulated Learning StrategiesJuan Hernández García100% (1)
- Piano Playing MechanismsDocument245 pagesPiano Playing MechanismsShawBoy2100% (1)
- Drawing Notes PDFDocument1 pageDrawing Notes PDFM.DalaniNo ratings yet
- Chapter 9 Voluntarism Structuralism and Other Early APDocument46 pagesChapter 9 Voluntarism Structuralism and Other Early APSyeda Farva50% (2)
- Bilingualism Cognitive Control Book Chapter-LibreDocument30 pagesBilingualism Cognitive Control Book Chapter-LibreHaliunaa BatboldNo ratings yet
- Selective mutism-DSM-5-233-235Document3 pagesSelective mutism-DSM-5-233-235Mella IntaniabellaNo ratings yet
- Unit 1: Testing and Assessment: 1.0 Learning OutcomesDocument14 pagesUnit 1: Testing and Assessment: 1.0 Learning OutcomesJoshua Miguel L. BarrosNo ratings yet
- Individual DifferencesDocument4 pagesIndividual Differences55-MBET-18No ratings yet
- The Stroop EffectDocument3 pagesThe Stroop EffectAndy CampbellNo ratings yet
- Notes On Language AcquisitionDocument3 pagesNotes On Language AcquisitionFrancis OpadaNo ratings yet
- Dce 3712 Conflict Resolution PowerpointDocument51 pagesDce 3712 Conflict Resolution PowerpointZahirul HaqNo ratings yet
- Revisiting Structural Family TherapyDocument2 pagesRevisiting Structural Family TherapyKim ScottNo ratings yet
- Ba 1 Sem 2 IntelligenceDocument40 pagesBa 1 Sem 2 IntelligenceKhushi Thapar100% (1)
- Psychology ExperimentDocument11 pagesPsychology ExperimentZunair IlyasNo ratings yet
- On Doing NothingDocument1 pageOn Doing NothingJerinNo ratings yet
- Meaning of ResearchDocument11 pagesMeaning of ResearchRahulNo ratings yet
- Question Paper Code: Reg. No.Document2 pagesQuestion Paper Code: Reg. No.gayathri nathNo ratings yet
- Social IssuesDocument7 pagesSocial IssuesNandya sankarNo ratings yet
- Research Methods in PsychologyDocument11 pagesResearch Methods in PsychologyJoe GattoNo ratings yet
- Personnel Psychology - 2006 - Judge - THE BIG FIVE PERSONALITY TRAITS GENERAL MENTAL ABILITY AND CAREER SUCCESS ACROSSDocument32 pagesPersonnel Psychology - 2006 - Judge - THE BIG FIVE PERSONALITY TRAITS GENERAL MENTAL ABILITY AND CAREER SUCCESS ACROSST LinNo ratings yet
- BPCC-109 em 2023-24-RDocument12 pagesBPCC-109 em 2023-24-Rmohnish aryanNo ratings yet
- HANDOUT Nine Temperament Traits Three Temperament TypesDocument2 pagesHANDOUT Nine Temperament Traits Three Temperament TypesQueenieNo ratings yet
- Psychology and Common Sense ArticleDocument12 pagesPsychology and Common Sense ArticleAdarsha DhakalNo ratings yet
- Social Influence & Group BehaviorDocument16 pagesSocial Influence & Group BehaviorPsyNo ratings yet
- Practical-1 Family Interview of An Unmarried AdultDocument9 pagesPractical-1 Family Interview of An Unmarried AdultKelly CevinNo ratings yet
- The Eclectic ApproachDocument1 pageThe Eclectic Approachcoolgame135No ratings yet
- Levels of ProcessingDocument15 pagesLevels of Processingkatherinepgirl100% (1)
- Historical Background of Educational PsychologyDocument18 pagesHistorical Background of Educational Psychologyburhan AhmedNo ratings yet
- ENG 508 HandoutsDocument114 pagesENG 508 Handoutsbani100% (1)
- Case History: By, Madhu Varma M.Phil. 1 Year NiepidDocument13 pagesCase History: By, Madhu Varma M.Phil. 1 Year Niepidsucess psychologyNo ratings yet
- Aggression Evolutionary PSYA3Document16 pagesAggression Evolutionary PSYA3careyallenNo ratings yet
- Academic Integrity AssignmentDocument3 pagesAcademic Integrity Assignmentapi-311850795No ratings yet
- NIMS Speech and Language Therapy Policy 18-19Document5 pagesNIMS Speech and Language Therapy Policy 18-19Fathima SNo ratings yet
- Interpersonal AttractionDocument13 pagesInterpersonal AttractionAkash Nagar100% (1)
- CH 09Document30 pagesCH 09kevinNo ratings yet
- Pschollinguistics - 5655Document24 pagesPschollinguistics - 5655Muhammad IbrahimNo ratings yet
- Speech Sound DisorderDocument2 pagesSpeech Sound DisorderVindo PurbaNo ratings yet
- Parallel Distributed ModelDocument4 pagesParallel Distributed ModelAnzala KhanNo ratings yet
- Edward Tolman (Sign Theory)Document3 pagesEdward Tolman (Sign Theory)Gie Marie Francisco UmaliNo ratings yet
- Article Review TemplateDocument5 pagesArticle Review TemplateMARIA AYUDIA ANINDHITANo ratings yet
- Classical ConditioningDocument18 pagesClassical ConditioningGraal GasparNo ratings yet
- Pgi ManualDocument5 pagesPgi ManualUrvashi100% (1)
- Dr. Ram Manohar Lohiya National Law University: PsychologyDocument4 pagesDr. Ram Manohar Lohiya National Law University: Psychologydivyavishal100% (1)
- Group 5 - CommunicationDisorder (Written Report)Document19 pagesGroup 5 - CommunicationDisorder (Written Report)Leo Angelo de CastroNo ratings yet
- NoamDocument6 pagesNoamNKECHINYEM BAKWENYENo ratings yet
- Learning CurvesDocument20 pagesLearning CurvesctoubiaNo ratings yet
- Stroop Effect TestDocument8 pagesStroop Effect TestSehaj BediNo ratings yet
- Case Study: Social Anxiety DisorderDocument13 pagesCase Study: Social Anxiety DisorderRohini RaghuNo ratings yet
- The in Uence of Superhero Comic Books On Adult Altruism: December 2016Document25 pagesThe in Uence of Superhero Comic Books On Adult Altruism: December 2016Claudio SanhuezaNo ratings yet
- Intellectual Development From Infancy To AdolescenceDocument19 pagesIntellectual Development From Infancy To AdolescenceJustin Chloe TorresNo ratings yet
- Learners With Reading ImpairmentDocument8 pagesLearners With Reading ImpairmentJinky OmboyNo ratings yet
- A Study On Language Disorders in Learners: December 2019Document9 pagesA Study On Language Disorders in Learners: December 2019msmsmsNo ratings yet
- Topic SentenceDocument7 pagesTopic SentenceFaridawati FiayNo ratings yet
- Types of Phrases in English: Intermediate Grammar: Phrase DevelopmentDocument7 pagesTypes of Phrases in English: Intermediate Grammar: Phrase DevelopmentFaridawati FiayNo ratings yet
- Students Teams-Achievement Divisions (STAD)Document4 pagesStudents Teams-Achievement Divisions (STAD)Faridawati FiayNo ratings yet
- ParaphrasingDocument12 pagesParaphrasingFaridawati FiayNo ratings yet
- Argumentative Essay Infotainment UseDocument1 pageArgumentative Essay Infotainment UseFaridawati FiayNo ratings yet
- Delimitation CommissionDocument3 pagesDelimitation CommissionNavraj Singh SahiNo ratings yet
- Interior Lightning SystemsDocument11 pagesInterior Lightning SystemsMedha GuptaNo ratings yet
- PEPA SummaryDocument6 pagesPEPA SummaryKhalid Masood GhaniNo ratings yet
- BrazilThe PROMINP Program PetrobrasDocument20 pagesBrazilThe PROMINP Program Petrobrask_fatahiNo ratings yet
- 27Document6 pages27Joanne FerrerNo ratings yet
- Game of Life The Fifth FlowerDocument146 pagesGame of Life The Fifth Flowersubto100% (1)
- From Disaster Response To Disaster Prevention Rachel Kyte at TEDxSendai EnglishDocument8 pagesFrom Disaster Response To Disaster Prevention Rachel Kyte at TEDxSendai EnglishDrenzel Vivencio33% (3)
- Example Road Pavement DesignDocument2 pagesExample Road Pavement Designnuraina aqilahNo ratings yet
- EDULIGHT Volume - 2, Issue - 4, Nov 2013Document278 pagesEDULIGHT Volume - 2, Issue - 4, Nov 2013EDULIGHT JOURNAL - A Peer Reviewed JournalNo ratings yet
- American Airlines Rainbow TeAAM and Its Strategy To Target The LGBT SegmentDocument25 pagesAmerican Airlines Rainbow TeAAM and Its Strategy To Target The LGBT SegmentManish ShawNo ratings yet
- Oct2011 Leather and Leather ProductsDocument12 pagesOct2011 Leather and Leather ProductsArif RamadhanNo ratings yet
- Introduction To Computer LanguagesDocument11 pagesIntroduction To Computer LanguagesHarsh ModiNo ratings yet
- Mayer Steel Pipe Corporation vs. Court of AppealsDocument9 pagesMayer Steel Pipe Corporation vs. Court of AppealsChristopher GunsatNo ratings yet
- Ikr17 RulesDocument52 pagesIkr17 RulesAnandNo ratings yet
- STRUCTURAL - CALC - FOR - GRANITE - CLADDING 1.5kpa R0 14 12 19 PDF 06 PDFDocument108 pagesSTRUCTURAL - CALC - FOR - GRANITE - CLADDING 1.5kpa R0 14 12 19 PDF 06 PDFmangeshNo ratings yet
- InterviewDocument2 pagesInterviewt3xxaNo ratings yet
- Carbonates IGCSE NotesDocument4 pagesCarbonates IGCSE NotesMisbah KamranNo ratings yet
- Telephone ConversationDocument2 pagesTelephone ConversationMJNo ratings yet
- Schemes of Maharashtra State Agricultural Marketing Board (Msamb)Document2 pagesSchemes of Maharashtra State Agricultural Marketing Board (Msamb)ChanakyaNo ratings yet
- 701018-Icea Uganda Money Market FundDocument1 page701018-Icea Uganda Money Market FundChrispus MutabuuzaNo ratings yet
- Heat Conduction Equation: Heat and Mass Transfer: Fundamentals & ApplicationsDocument75 pagesHeat Conduction Equation: Heat and Mass Transfer: Fundamentals & Applicationssalim ekizNo ratings yet
- Term Paper About FreedomDocument6 pagesTerm Paper About Freedomea4gaa0g100% (1)
- The Cask of Amontillado (Summary)Document5 pagesThe Cask of Amontillado (Summary)Ria LopezNo ratings yet
- Protecting The Marine EnvironmentDocument13 pagesProtecting The Marine EnvironmentCirilo Aguadera Lagnason Jr.No ratings yet
- Layers of EarthDocument13 pagesLayers of EarthJazrel D. De Los SantosNo ratings yet