You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Ultimate Science-Based Supplement GuideDocument25 pagesThe Ultimate Science-Based Supplement GuideSean85% (13)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Berkhan's Leangains PDFDocument1 pageBerkhan's Leangains PDFferncaz95No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Build Muscle CalisthenicsDocument83 pagesBuild Muscle CalisthenicsPedro Vasconcelos71% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4 Nutrition in InfancyDocument92 pages4 Nutrition in InfancyramszlaiNo ratings yet
- 2019 DaveyFisher Cutting NutritionProgramDocument30 pages2019 DaveyFisher Cutting NutritionProgramJonathan NguyenNo ratings yet
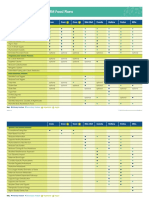
- 7ilZ0x4T5Msm1NbH - DjzOqev81 - NCJZ9 09 Features of The IFM Food Plans - One SheetDocument2 pages7ilZ0x4T5Msm1NbH - DjzOqev81 - NCJZ9 09 Features of The IFM Food Plans - One SheetRaghda AlawadiNo ratings yet
- Technological Institute of The Philippines - Quezon City Physical Education Department Phsyical Fitness Test Scoring For Prelims (Pathfit 1&2)Document4 pagesTechnological Institute of The Philippines - Quezon City Physical Education Department Phsyical Fitness Test Scoring For Prelims (Pathfit 1&2)JenalineBalderosaNo ratings yet
- 8 Effective Tips To Lose Fat in Your FaceDocument6 pages8 Effective Tips To Lose Fat in Your Facehamrani karim100% (1)
- Diet For Cardiovascular DisordersDocument7 pagesDiet For Cardiovascular Disordersshannon c. lewisNo ratings yet
- Level 2 Food Hygiene and Safety For Catering: Course Content OverviewDocument4 pagesLevel 2 Food Hygiene and Safety For Catering: Course Content Overviewraja100% (1)
- Physical Fitness Test FormDocument3 pagesPhysical Fitness Test FormAnthony Gerarld TalainNo ratings yet
- Chapter 5 HandoutDocument4 pagesChapter 5 Handouttrixie eustaquioNo ratings yet
- Obesity in Children Adolescents.20Document10 pagesObesity in Children Adolescents.20Naga LakshmiNo ratings yet
- Products by Body Benefit - Total Body HealthDocument7 pagesProducts by Body Benefit - Total Body HealthShehera Fallan NovoNo ratings yet
- Community Care PlanDocument6 pagesCommunity Care PlanKristian Dave DivaNo ratings yet
- Health LessonDocument2 pagesHealth Lessonapi-279619852No ratings yet
- Watermelon 2Document2 pagesWatermelon 2Wania ShahidNo ratings yet
- Nutrition and Digestion Case Study Lesson 1Document2 pagesNutrition and Digestion Case Study Lesson 1api-209270909No ratings yet
- Tips To Get Rid of DiabetesDocument16 pagesTips To Get Rid of DiabetesPriyankaNo ratings yet
- Remedial Measures of Health and Safty in Textile Industry: PREPARED BY: F. Islam Surjo DuetDocument26 pagesRemedial Measures of Health and Safty in Textile Industry: PREPARED BY: F. Islam Surjo DuetTextile Engineers Association of BholaNo ratings yet
- Biology Investigatory 2.o KKDocument19 pagesBiology Investigatory 2.o KKK GhatageNo ratings yet
- 8 Best Cardio Workouts You Can Do at Home - Meritage Medical Network PDFDocument7 pages8 Best Cardio Workouts You Can Do at Home - Meritage Medical Network PDFyoucef mohamed100% (1)
- Components of Food-PPT-6: Prasanta ChoudhuryDocument13 pagesComponents of Food-PPT-6: Prasanta ChoudhuryOdol PranavNo ratings yet
- AQI Bulletin 20201126Document10 pagesAQI Bulletin 20201126Kartik PrabhakarNo ratings yet
- Multigrain Flour - Article.editedDocument7 pagesMultigrain Flour - Article.editedMuqadas AzizNo ratings yet
- NCPDocument2 pagesNCPGlenn CabradillaNo ratings yet
- Dietary Manual Ali Bin Ali Hospital, 2021Document55 pagesDietary Manual Ali Bin Ali Hospital, 2021mayadaformoNo ratings yet
- Body CalculatorsDocument85 pagesBody CalculatorsGaurav AroraNo ratings yet
- Template For Action Plan 2Document2 pagesTemplate For Action Plan 2Mhartin OrsalNo ratings yet
- Exercise PracticeDocument5 pagesExercise PracticeLương PhượngNo ratings yet