You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Blacklight Mutator PDFDocument10 pagesBlacklight Mutator PDFBruce WilliamsNo ratings yet
- Illumina Covidseq Ruo Kits Reference Guide 1000000126053 08Document39 pagesIllumina Covidseq Ruo Kits Reference Guide 1000000126053 08Íris terezinhaNo ratings yet
- Swine Flu WhitepaperDocument95 pagesSwine Flu WhitepaperPatrick Savalle100% (1)
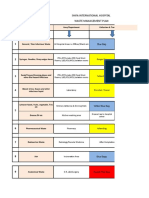
- Shifa International Hospital Waste Management PlanDocument6 pagesShifa International Hospital Waste Management PlanAhmed UmerNo ratings yet
- Toxoplasma GondiiDocument6 pagesToxoplasma GondiiSyawal HariadiNo ratings yet
- Fidic Policies New Series 1 5Document23 pagesFidic Policies New Series 1 5codefinderNo ratings yet
- Week 3 4 Modules 8subjects PDFDocument139 pagesWeek 3 4 Modules 8subjects PDFmae KuanNo ratings yet
- ENLS V4.0 ME Manuscript FINALDocument17 pagesENLS V4.0 ME Manuscript FINALkoko komarudinNo ratings yet
- Paper 2nd YearDocument7 pagesPaper 2nd Yeartalibh577No ratings yet
- Immunisation Against Infectious Disease (2006)Document516 pagesImmunisation Against Infectious Disease (2006)pasko100% (1)
- Microbiology and Immunology Pokhara University Syllabus NOCDocument2 pagesMicrobiology and Immunology Pokhara University Syllabus NOCDinesh SubediNo ratings yet
- Lesson 01 Present Simple HomeworkDocument5 pagesLesson 01 Present Simple HomeworkAhmed EltohamyNo ratings yet
- NCLEXDocument10 pagesNCLEXApril Kirstin ChuaNo ratings yet
- BAM Chapter 18 - Yeasts, Molds and Mycotoxins - FDADocument13 pagesBAM Chapter 18 - Yeasts, Molds and Mycotoxins - FDAsunnysatwNo ratings yet
- English7 LAS 5 Week 5Document10 pagesEnglish7 LAS 5 Week 5Edmond GalvezNo ratings yet
- Torch InfectionsDocument27 pagesTorch InfectionsSimi SaiPrasoonNo ratings yet
- Service Manual For XL-300 With ISE-V2019.01Document533 pagesService Manual For XL-300 With ISE-V2019.01grand laboNo ratings yet
- Saponinas PDFDocument4 pagesSaponinas PDFJohnny Saavedra CamachoNo ratings yet
- Test Bank For Microbiology With Diseases Body System 3rd Edition BaumanDocument21 pagesTest Bank For Microbiology With Diseases Body System 3rd Edition BaumanStan Mcclellan100% (28)
- Diet Therapy 1Document2 pagesDiet Therapy 1christine gisembaNo ratings yet
- Sample Questions: A Collective Arrangement by The Chapter Editors, Associate Editors, and CD-ROM Editor of 2005Document38 pagesSample Questions: A Collective Arrangement by The Chapter Editors, Associate Editors, and CD-ROM Editor of 2005Jennifer Schymick100% (2)
- Biological Hazards Epidemics and Pandemics Science Presentation in Colorful Cartoon StyleDocument13 pagesBiological Hazards Epidemics and Pandemics Science Presentation in Colorful Cartoon StyleMacky VelascoNo ratings yet
- Sterilization in Orthodontics-A Review: International Journal of Current Research September 2016Document5 pagesSterilization in Orthodontics-A Review: International Journal of Current Research September 2016Sulvina MaradewiNo ratings yet
- The Mind Body Interaction in DiseaseDocument8 pagesThe Mind Body Interaction in DiseaseYuli MSNo ratings yet
- Expanded Program Immunization: NCM 104: Community Health Nursing I: Individual and FamilyDocument25 pagesExpanded Program Immunization: NCM 104: Community Health Nursing I: Individual and FamilyRica machells DaydaNo ratings yet
- Provision of A Safe EnvironmentDocument19 pagesProvision of A Safe EnvironmentKristian Jane de JesusNo ratings yet
- tmpC737 TMPDocument277 pagestmpC737 TMPFrontiersNo ratings yet
- Zhang Et Al., 2020Document2 pagesZhang Et Al., 2020camil fernandezNo ratings yet
- ข้อสอบเข้ามหาวิทยาลัย ภาษาอังกฤษ (2532) ชุดที่Document14 pagesข้อสอบเข้ามหาวิทยาลัย ภาษาอังกฤษ (2532) ชุดที่littleusa bykrukapookNo ratings yet
- JIBACHHAAPPLIEDPREVENTIVEVETERINARYMEDICINEresearchgateDocument25 pagesJIBACHHAAPPLIEDPREVENTIVEVETERINARYMEDICINEresearchgatesoham samantaNo ratings yet