You might also like
- Cardiac DrugsDocument10 pagesCardiac DrugsNursePoor98% (47)
- Cardiac Failure: Definition: Compensatory Changes in Heart FailureDocument5 pagesCardiac Failure: Definition: Compensatory Changes in Heart FailureMatyie SmkasNo ratings yet
- Blueprints Primary Care TablesDocument40 pagesBlueprints Primary Care TablesAnne Lowry92% (13)
- Handbook of AnesthesiologyDocument176 pagesHandbook of AnesthesiologyarmelzahfauziNo ratings yet
- ACLS MneumonicsDocument4 pagesACLS MneumonicsnaranothNo ratings yet
- Percutaneous InterventionsDocument55 pagesPercutaneous InterventionsShannon Bellamy-FoggNo ratings yet
- Cardiac Arrythmias in The ED Menbeu Edited From AnaDocument106 pagesCardiac Arrythmias in The ED Menbeu Edited From AnaTemesgen Geleta100% (1)
- ACLS Algorithms SlideDocument26 pagesACLS Algorithms SlidehrsoNo ratings yet
- ACLS Tachycardia Algorithm For Managing Unstable TachycardiaDocument2 pagesACLS Tachycardia Algorithm For Managing Unstable TachycardiaLady MuffinsNo ratings yet
- Pro32 SupraventricularTachycardiaDocument1 pagePro32 SupraventricularTachycardiaRonald KendallNo ratings yet
- Assessment of The Acutely Ill PatientDocument10 pagesAssessment of The Acutely Ill PatientZacmilo Dela TorreNo ratings yet
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki HartawanNo ratings yet
- Pulmonary HTNDocument51 pagesPulmonary HTNMuhammad HaekalNo ratings yet
- Hemodynamics Basic Concepts 1204053445109897 4Document115 pagesHemodynamics Basic Concepts 1204053445109897 4valeriesolidum100% (1)
- Tachyarrhythmias When Should I Refer?Document25 pagesTachyarrhythmias When Should I Refer?Cindy Seow Sieng TengNo ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- Lecture - 2 Advanced Cardiac Life SupportDocument28 pagesLecture - 2 Advanced Cardiac Life SupportJixon GeorgeNo ratings yet
- Arrhythmic PatientsDocument15 pagesArrhythmic PatientsBen ScottNo ratings yet
- Peri Arrest ArrhythmiasDocument40 pagesPeri Arrest ArrhythmiasDestiAriyaniNo ratings yet
- Management of Symptomatic Bradycardia and TachycardiaDocument55 pagesManagement of Symptomatic Bradycardia and TachycardiaDewintha Airene NoviantiNo ratings yet
- CHFalgorithm Univ of MSDocument1 pageCHFalgorithm Univ of MSDominique Excelsis J. DegamoNo ratings yet
- Tachy/賸)Document28 pagesTachy/賸)Jason LinNo ratings yet
- Sample Medical Guidelines: ACLS-BradycardiaDocument2 pagesSample Medical Guidelines: ACLS-BradycardiaCheewin KhawprapaNo ratings yet
- Ecg NotesDocument16 pagesEcg NotesAszhiNo ratings yet
- Atrial Fibrillation: Dr. Zirath + Dr. MehtaDocument29 pagesAtrial Fibrillation: Dr. Zirath + Dr. MehtaAjayNo ratings yet
- Synthesis: History Report SBAR Complete PA Know Your Patho!!! Don't Get Caught W/drawersDocument30 pagesSynthesis: History Report SBAR Complete PA Know Your Patho!!! Don't Get Caught W/drawersmmcgee002No ratings yet
- ACLS-Pediatric Wide Complex Tachycardia: Sample Medical GuidelinesDocument2 pagesACLS-Pediatric Wide Complex Tachycardia: Sample Medical GuidelinesFebrialitaFatoniNo ratings yet
- Pulseless Arrest Algorythm: Symptoms PersistDocument1 pagePulseless Arrest Algorythm: Symptoms PersistMeita ReligiaNo ratings yet
- Hypertensive Emergency: Beny Ghufron Dept. of Internal Medicine June 2011Document31 pagesHypertensive Emergency: Beny Ghufron Dept. of Internal Medicine June 2011Dendian Berlia JelitaNo ratings yet
- Crisis of Hypertension Revised 1Document57 pagesCrisis of Hypertension Revised 1Ratna Puspa RahayuNo ratings yet
- Arrhythmia 3Document2 pagesArrhythmia 3Nikey LimNo ratings yet
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Arrhythmias: Nightfloat Curriculum 2010-2011 LPCH Pediatric Residency ProgramDocument26 pagesArrhythmias: Nightfloat Curriculum 2010-2011 LPCH Pediatric Residency Programkamel6No ratings yet
- Atrial Dysrhythmias: Etiology, Physical Assessment, and TreatmentDocument2 pagesAtrial Dysrhythmias: Etiology, Physical Assessment, and TreatmentMelissaNo ratings yet
- Acute HFDocument36 pagesAcute HFeman roshdyNo ratings yet
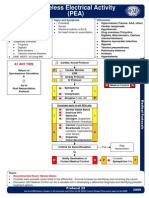
- Pro29 PulselessElectricalActivityDocument1 pagePro29 PulselessElectricalActivityZen Firhan ShahabNo ratings yet
- Think Link Ecg Notes: Normal Sinus Rhythm at 70 Beats/minDocument3 pagesThink Link Ecg Notes: Normal Sinus Rhythm at 70 Beats/minWillington CuaresmaNo ratings yet
- Chest PainDocument2 pagesChest PaindrsmiNo ratings yet
- Chapter3Shock CirculationDocument13 pagesChapter3Shock CirculationSri AgustinaNo ratings yet
- Pulmonary Hypertension - LITFL - CCC CardiologyDocument1 pagePulmonary Hypertension - LITFL - CCC CardiologymyaqanithaNo ratings yet
- Vasopressors: Jennifer & Joshua Chalk Talk 1/17/2014 Go Hawks!Document44 pagesVasopressors: Jennifer & Joshua Chalk Talk 1/17/2014 Go Hawks!pattumkp100% (1)
- Reviewer For DutyDocument4 pagesReviewer For DutyBenedict James BermasNo ratings yet
- Final Copy HTN EmergencyDocument13 pagesFinal Copy HTN EmergencyabrarNo ratings yet
- Arrhythmias: Domina Petric, MDDocument22 pagesArrhythmias: Domina Petric, MDMwaba PeterNo ratings yet
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument64 pagesDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyNo ratings yet
- Approach To Tachyarrhythmia: SVT - VT - VF - Torsa de PointesDocument17 pagesApproach To Tachyarrhythmia: SVT - VT - VF - Torsa de PointesAmir Izzuddin SuibNo ratings yet
- Pharm Final ReviewDocument8 pagesPharm Final ReviewKasey C. PintoNo ratings yet
- ATrial FibrillationDocument21 pagesATrial FibrillationMohammad Farouq OmarNo ratings yet
- Approach To Dyspnea: Dr. Ghulam Hussain Baloch Associate Professor of Medicine LUMHS, JamshoroDocument48 pagesApproach To Dyspnea: Dr. Ghulam Hussain Baloch Associate Professor of Medicine LUMHS, JamshoroAndita Delifauzan SyabanaNo ratings yet
- 6 BradycardiaDocument20 pages6 BradycardiaTejas Vivek WaghNo ratings yet
- Treatment Protocol For Hypertension: Criteria For Diagnosing High Blood PressureDocument3 pagesTreatment Protocol For Hypertension: Criteria For Diagnosing High Blood PressureHarshitha LokeshNo ratings yet
- Acls TachiDocument1 pageAcls TachiratnawkNo ratings yet
- Dysrhythmias NotesDocument23 pagesDysrhythmias NoteskmimmackNo ratings yet
- Cardiology FMDocument25 pagesCardiology FMtrushaNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Guide to Canine and Feline ElectrocardiographyFrom EverandGuide to Canine and Feline ElectrocardiographyRuth WillisNo ratings yet
- Daftar Pustaka PreliminaryDocument1 pageDaftar Pustaka Preliminarychr0m3b4tm4nNo ratings yet
- BoaDocument2 pagesBoachr0m3b4tm4nNo ratings yet
- ExoDocument1 pageExochr0m3b4tm4nNo ratings yet
- 1Document3 pages1nikojoeNo ratings yet
- LuisDocument3 pagesLuischr0m3b4tm4nNo ratings yet
- ExoDocument2 pagesExochr0m3b4tm4nNo ratings yet
- ExoDocument1 pageExochr0m3b4tm4nNo ratings yet
- SubmarineDocument1 pageSubmarinechr0m3b4tm4nNo ratings yet
- ExoDocument2 pagesExochr0m3b4tm4nNo ratings yet
- ExoDocument1 pageExochr0m3b4tm4nNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakachr0m3b4tm4nNo ratings yet
- DenadaDocument3 pagesDenadachr0m3b4tm4nNo ratings yet
- New Text DocumentDocument1 pageNew Text Documentchr0m3b4tm4nNo ratings yet
- New Text DocumentDocument1 pageNew Text Documentchr0m3b4tm4nNo ratings yet
- BOTRDocument1 pageBOTRchr0m3b4tm4nNo ratings yet
- Atrial Fibrillation: The Most Common ArrhythmiaDocument2 pagesAtrial Fibrillation: The Most Common Arrhythmiachr0m3b4tm4nNo ratings yet
- 14 CTN CelebiDocument3 pages14 CTN Celebichr0m3b4tm4nNo ratings yet
- Pi Catheter Ablation Ventricular TachycardiaDocument16 pagesPi Catheter Ablation Ventricular Tachycardiachr0m3b4tm4nNo ratings yet
- Atrial Fibrillation: The Most Common ArrhythmiaDocument2 pagesAtrial Fibrillation: The Most Common Arrhythmiachr0m3b4tm4nNo ratings yet
- TachalgoDocument1 pageTachalgochr0m3b4tm4nNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakachr0m3b4tm4nNo ratings yet
- Ellie Goulding Love Me Like You DoDocument1 pageEllie Goulding Love Me Like You Dochr0m3b4tm4nNo ratings yet
- Dora Dora - Alex MicaDocument2 pagesDora Dora - Alex Micachr0m3b4tm4nNo ratings yet
- Imagine Dragon - DemonsDocument2 pagesImagine Dragon - Demonschr0m3b4tm4nNo ratings yet