You might also like
- ACLS Pocket CardDocument6 pagesACLS Pocket Cardno_spam_mang80% (5)
- EKG Findings and Arrhythmias - USMLE Step 2 CK ExamDocument3 pagesEKG Findings and Arrhythmias - USMLE Step 2 CK ExamSamah Khan100% (2)
- ACLS (Advanced Cardiac Life Support) Algorithms & NotesDocument4 pagesACLS (Advanced Cardiac Life Support) Algorithms & Notesiamlucil100% (4)
- Tachycardia Algorithm A0Document1 pageTachycardia Algorithm A0Ene ElenaNo ratings yet
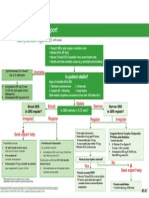
- Adult Tachycardia Algorithm: (With Pulse)Document1 pageAdult Tachycardia Algorithm: (With Pulse)ITSimplyNo ratings yet
- Adult Tachycardia Algorithm: (With Pulse)Document1 pageAdult Tachycardia Algorithm: (With Pulse)ITSimplyNo ratings yet
- Adult Tachycardia Algorithm: (With Pulse)Document1 pageAdult Tachycardia Algorithm: (With Pulse)Mohammed AhmedNo ratings yet
- Management of Cardiac Arrhytmia in Advanced Cardiac Life Support (ACLS)Document34 pagesManagement of Cardiac Arrhytmia in Advanced Cardiac Life Support (ACLS)rhezzaagxxNo ratings yet
- Basic ECG For ParamedicDocument82 pagesBasic ECG For ParamedicMaza AmfoterikNo ratings yet
- ArrhythmiasDocument47 pagesArrhythmiasJaismi AntonyNo ratings yet
- Arrhythmia Overview: Antonia Anna LukitoDocument45 pagesArrhythmia Overview: Antonia Anna LukitoJoshua ObrienNo ratings yet
- Tatalaksana ArrthytmiaDocument55 pagesTatalaksana ArrthytmiaJanstine FirstiandyNo ratings yet
- ECG MonitoringDocument96 pagesECG MonitoringJey BautistaNo ratings yet
- Basic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCDocument42 pagesBasic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCtuffie85No ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- DC Shock + AritmiaDocument34 pagesDC Shock + AritmiaSuparno Adi SantikaNo ratings yet
- Gamal Abd EL Nasser Mahmoud: Prepared ByDocument64 pagesGamal Abd EL Nasser Mahmoud: Prepared ByMohamed ElkadyNo ratings yet
- Brady ArrhythmiasDocument36 pagesBrady ArrhythmiasSajin AlexanderNo ratings yet
- Approach To Tachyarrhythmia: SVT - VT - VF - Torsa de PointesDocument17 pagesApproach To Tachyarrhythmia: SVT - VT - VF - Torsa de PointesAmir Izzuddin SuibNo ratings yet
- Ekg PsikDocument69 pagesEkg PsikZEISVA APRILIANINGRUMNo ratings yet
- Aritmia LetalDocument53 pagesAritmia LetalMetta SariNo ratings yet
- 10 Peri Arrest ArrhythmiasDocument39 pages10 Peri Arrest ArrhythmiasAnaid FourevaNo ratings yet
- EKG StripsDocument10 pagesEKG StripsSaidel ElizondoNo ratings yet
- 24hr ECG InterpretationDocument26 pages24hr ECG InterpretationMariaNo ratings yet
- Arrhythmia NewDocument73 pagesArrhythmia Newlohith saiNo ratings yet
- Hippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2Document10 pagesHippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2alexandertorresreyNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- Cases in Emergency 2 PDFDocument6 pagesCases in Emergency 2 PDFAndreea MihaelaNo ratings yet
- Normal ECG: - P Wave: Between 3 - 5 Little Square - Lead V1 Is A Good Place To StartDocument80 pagesNormal ECG: - P Wave: Between 3 - 5 Little Square - Lead V1 Is A Good Place To Startkuchniaat123No ratings yet
- APS (Autosaved)Document15 pagesAPS (Autosaved)Anita ReveraNo ratings yet
- Aritmia LetalDocument49 pagesAritmia LetalfebriyakNo ratings yet
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Supplementary Material 4.3 Cardiac Rhythm Disorders-2Document14 pagesSupplementary Material 4.3 Cardiac Rhythm Disorders-2Andrea Love PalomoNo ratings yet
- Chapter 4e Internal MedicineDocument19 pagesChapter 4e Internal MedicinepodmmgfNo ratings yet
- Ecgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaDocument47 pagesEcgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaAuliaRusdiAllmuttaqienNo ratings yet
- Basic ECG Interpretation - LeonardDocument33 pagesBasic ECG Interpretation - LeonardAyen FornollesNo ratings yet
- ECG UpdatedDocument115 pagesECG Updatedmominarasool7No ratings yet
- 5 Tachycardias With PulseDocument27 pages5 Tachycardias With PulseTejas Vivek WaghNo ratings yet
- Supraventricular Tachycardia: Presented by Normadihah Binti Mohd Zainuddin BolekDocument11 pagesSupraventricular Tachycardia: Presented by Normadihah Binti Mohd Zainuddin BolekmadiehahNo ratings yet
- Cardiology Notes USMLE Step CKDocument135 pagesCardiology Notes USMLE Step CKArianna BetancourtNo ratings yet
- ECG Intro With Ref To QT Interval FinalDocument59 pagesECG Intro With Ref To QT Interval FinalGeorge VergheseNo ratings yet
- Myocardial InfarctionDocument39 pagesMyocardial InfarctionYauffa Hanna Elt MisykahNo ratings yet
- PALS - Rhythm Disturbance 02Document27 pagesPALS - Rhythm Disturbance 02Rich AdamsNo ratings yet
- U.M.F. "Gr. T. Popa" Ia Ş IDocument37 pagesU.M.F. "Gr. T. Popa" Ia Ş Ij.doe.hex_87No ratings yet
- ECG3Document58 pagesECG3Plzstudylav SyedNo ratings yet
- Angina Nursing STIKESDocument44 pagesAngina Nursing STIKESminikompoNo ratings yet
- Er FinalsDocument63 pagesEr FinalsNaren RaviNo ratings yet
- Angina Pectoris 2Document47 pagesAngina Pectoris 2inyanji.barasaNo ratings yet
- 0 Arrhythmia Arwin PDFDocument53 pages0 Arrhythmia Arwin PDFEvans HansenNo ratings yet
- Ischaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeDocument104 pagesIschaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeputriluftiNo ratings yet
- Introduction To Electrophysiology: What Are They DOING Over There?!Document51 pagesIntroduction To Electrophysiology: What Are They DOING Over There?!Mahendrakumar ManiNo ratings yet
- TachycardiaDocument7 pagesTachycardiaArvind SahniNo ratings yet
- Acls TachiDocument1 pageAcls TachiratnawkNo ratings yet
- Easy EKGDocument45 pagesEasy EKGnov14No ratings yet
- ECG Monitoring and Rhythm RecognitionDocument36 pagesECG Monitoring and Rhythm Recognitionمحمد زينNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Guide to Canine and Feline ElectrocardiographyFrom EverandGuide to Canine and Feline ElectrocardiographyRuth WillisNo ratings yet
- Daftar Pustaka PreliminaryDocument1 pageDaftar Pustaka Preliminarychr0m3b4tm4nNo ratings yet
- BoaDocument2 pagesBoachr0m3b4tm4nNo ratings yet
- ExoDocument1 pageExochr0m3b4tm4nNo ratings yet
- 1Document3 pages1nikojoeNo ratings yet
- LuisDocument3 pagesLuischr0m3b4tm4nNo ratings yet
- ExoDocument2 pagesExochr0m3b4tm4nNo ratings yet
- ExoDocument1 pageExochr0m3b4tm4nNo ratings yet
- SubmarineDocument1 pageSubmarinechr0m3b4tm4nNo ratings yet
- ExoDocument2 pagesExochr0m3b4tm4nNo ratings yet
- ExoDocument1 pageExochr0m3b4tm4nNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakachr0m3b4tm4nNo ratings yet
- DenadaDocument3 pagesDenadachr0m3b4tm4nNo ratings yet
- New Text DocumentDocument1 pageNew Text Documentchr0m3b4tm4nNo ratings yet
- New Text DocumentDocument1 pageNew Text Documentchr0m3b4tm4nNo ratings yet
- BOTRDocument1 pageBOTRchr0m3b4tm4nNo ratings yet
- Atrial Fibrillation: The Most Common ArrhythmiaDocument2 pagesAtrial Fibrillation: The Most Common Arrhythmiachr0m3b4tm4nNo ratings yet
- 14 CTN CelebiDocument3 pages14 CTN Celebichr0m3b4tm4nNo ratings yet
- Ventricular Tachycardia: History Signs and Symptoms DifferentialDocument1 pageVentricular Tachycardia: History Signs and Symptoms Differentialchr0m3b4tm4nNo ratings yet
- Atrial Fibrillation: The Most Common ArrhythmiaDocument2 pagesAtrial Fibrillation: The Most Common Arrhythmiachr0m3b4tm4nNo ratings yet
- Pi Catheter Ablation Ventricular TachycardiaDocument16 pagesPi Catheter Ablation Ventricular Tachycardiachr0m3b4tm4nNo ratings yet
- Daftar PustakaDocument1 pageDaftar Pustakachr0m3b4tm4nNo ratings yet
- Ellie Goulding Love Me Like You DoDocument1 pageEllie Goulding Love Me Like You Dochr0m3b4tm4nNo ratings yet
- Dora Dora - Alex MicaDocument2 pagesDora Dora - Alex Micachr0m3b4tm4nNo ratings yet
- Imagine Dragon - DemonsDocument2 pagesImagine Dragon - Demonschr0m3b4tm4nNo ratings yet