You might also like
- NATIONAL GUIDELINES ON QUALITY OBSTETRICS AND PERINATAL CARE Final Feb 2022 PDFDocument700 pagesNATIONAL GUIDELINES ON QUALITY OBSTETRICS AND PERINATAL CARE Final Feb 2022 PDFvincent obunga50% (2)
- ACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Document15 pagesACOG SMFM Joint Practice Bulletin Multiple Gestation 2004Reza ZulkarnainNo ratings yet
- FSRH Guidance Switching or Starting Methods of Contraception August 2019Document10 pagesFSRH Guidance Switching or Starting Methods of Contraception August 2019Ting Yiu WongNo ratings yet
- Fetal Medicine - Bidyut KumarDocument4 pagesFetal Medicine - Bidyut KumarpatoxyzuNo ratings yet
- Acog Practice Bulletin: Thromboembolism in PregnancyDocument17 pagesAcog Practice Bulletin: Thromboembolism in PregnancytriNo ratings yet
- ACOG Practice Bulletin No163Document15 pagesACOG Practice Bulletin No163Marco DiestraNo ratings yet
- UNAS Nov 2019Document25 pagesUNAS Nov 2019paramitastellaNo ratings yet
- Gallstones in Pregnancy - UpToDateDocument51 pagesGallstones in Pregnancy - UpToDateLeira BarbosaNo ratings yet
- ACOG Bulletin MiscarriageDocument12 pagesACOG Bulletin Miscarriagebrabba19856403No ratings yet
- AACE/ACE Disease State Clinical ReviewDocument10 pagesAACE/ACE Disease State Clinical ReviewSanjay NavaleNo ratings yet
- Diabetes Acog 2017Document15 pagesDiabetes Acog 2017Holger Vicente Guerrero Guerrero100% (1)
- Acog Practice Bulletin: Pregnancy and Heart DiseaseDocument37 pagesAcog Practice Bulletin: Pregnancy and Heart Diseasereham mohamedNo ratings yet
- Acog SDR AntifosfolipidicDocument8 pagesAcog SDR Antifosfolipidicleonar8No ratings yet
- Acog Practice Bulletin: Pregestational Diabetes MellitusDocument21 pagesAcog Practice Bulletin: Pregestational Diabetes MellitusGia DuyNo ratings yet
- Acog - Practice Bulletin Gynecology PDFDocument486 pagesAcog - Practice Bulletin Gynecology PDFali alrashediNo ratings yet
- Poly Hi DR AmnionDocument7 pagesPoly Hi DR Amnionwanwan_adongNo ratings yet
- Practice Bulletin: Antiphospholipid SyndromeDocument8 pagesPractice Bulletin: Antiphospholipid SyndromeSus ArNo ratings yet
- Leiomioma - TratamientoDocument37 pagesLeiomioma - TratamientoNella SolanoNo ratings yet
- Unas November 2019Document21 pagesUnas November 2019Muhammad FaisalNo ratings yet
- Dysmenorrhoea in Adult WomenDocument16 pagesDysmenorrhoea in Adult Womenfarmasi_hm100% (1)
- ACOG Practice Bulletin No. 202 - Hipertensión Gestacional y ... - Obstetricia y Ginecología PDFDocument36 pagesACOG Practice Bulletin No. 202 - Hipertensión Gestacional y ... - Obstetricia y Ginecología PDFAnghelino Jesus Meza CentenoNo ratings yet
- Gyne LE 2: Stage IVA Is Characterized byDocument49 pagesGyne LE 2: Stage IVA Is Characterized byĐinesh IlavarasanNo ratings yet
- Acog 19Document25 pagesAcog 19Janet GoldameirNo ratings yet
- ACOG Tech BullitinDocument20 pagesACOG Tech BullitinJosephNo ratings yet
- Gestational Trophoblastic DiseaseDocument6 pagesGestational Trophoblastic DiseaseSJ IraaNo ratings yet
- Acog 194Document15 pagesAcog 194Marco DiestraNo ratings yet
- Blood Transfusiopn in Obstetrics (RCOG, May 2015) PDFDocument23 pagesBlood Transfusiopn in Obstetrics (RCOG, May 2015) PDFwebcob246No ratings yet
- (SLE) and PregnancyDocument60 pages(SLE) and PregnancyNurfikhaHandayaniNo ratings yet
- 46 60Document7 pages46 60member12dNo ratings yet
- Dystocia and Augmentation of LAbor PDFDocument10 pagesDystocia and Augmentation of LAbor PDFKathleen100% (1)
- Acute Uterine InversionDocument6 pagesAcute Uterine InversionBima GhovaroliyNo ratings yet
- Incorrects On NBME ObgynDocument4 pagesIncorrects On NBME Obgynkabal321No ratings yet
- Acog 2019 Preeclampsia PDFDocument25 pagesAcog 2019 Preeclampsia PDFJhoel Zuñiga LunaNo ratings yet
- App 2021 AcogDocument26 pagesApp 2021 AcogFernanda Copete Yolianis100% (1)
- TC11Document4 pagesTC11FrancisNo ratings yet
- Cardiac Disease and Pregnancy RCOG GuidelineDocument18 pagesCardiac Disease and Pregnancy RCOG GuidelinedanielsusenoNo ratings yet
- Gestational Diabetes MellitusDocument73 pagesGestational Diabetes Mellitusreniere lagazoNo ratings yet
- Mucinous Cystadenoma 0708Document12 pagesMucinous Cystadenoma 0708eosfieldNo ratings yet
- Hemorragia Posparto-AcogDocument19 pagesHemorragia Posparto-AcogCristian LaraNo ratings yet
- RCOG Guideline 2011Document24 pagesRCOG Guideline 2011John DoeNo ratings yet
- ACOG Management of Stillbirth PDFDocument14 pagesACOG Management of Stillbirth PDFLêMinhĐứcNo ratings yet
- TOG Online SBA Resource, Vol. 20 Issue 2Document6 pagesTOG Online SBA Resource, Vol. 20 Issue 2FA KhanNo ratings yet
- Revision Long Case Obs GynaeDocument10 pagesRevision Long Case Obs GynaeHo Yong WaiNo ratings yet
- Practice Test: Order Your Manuals NowDocument31 pagesPractice Test: Order Your Manuals NowTadele DerbewNo ratings yet
- ACOG Fetal Maturity Guidelines PDFDocument8 pagesACOG Fetal Maturity Guidelines PDFinayahsyNo ratings yet
- RCOG - Management of Suspected Ovarian Masses in Premenopausal WomenDocument14 pagesRCOG - Management of Suspected Ovarian Masses in Premenopausal Womenestridente81No ratings yet
- Rcog PretermDocument13 pagesRcog Pretermsintiadamayanti100% (1)
- ACOG Abnormal Uterine Bleeding DiagnosisDocument11 pagesACOG Abnormal Uterine Bleeding DiagnosisJimmy Crack CornsNo ratings yet
- TOG Myocardial Infarction and PregnancyDocument9 pagesTOG Myocardial Infarction and PregnancyMarNo ratings yet
- Hipertensión en El Embarazo ACOG2013Document10 pagesHipertensión en El Embarazo ACOG2013Ramiro Castro ApoloNo ratings yet
- Hypertension in PregnancyDocument15 pagesHypertension in PregnancyLaura María Salamanca Ternera0% (1)
- Literature Review Hypertension in PregnancyDocument7 pagesLiterature Review Hypertension in Pregnancyafmzsprjlerxio100% (1)
- Endoscopic Intervention and Cholecystectomy in Pregnant Women With Acute Biliary Pancreatitis Decreases Early ReadmissionsDocument19 pagesEndoscopic Intervention and Cholecystectomy in Pregnant Women With Acute Biliary Pancreatitis Decreases Early ReadmissionsCarlos Altez FernandezNo ratings yet
- Update On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal MedicineDocument217 pagesUpdate On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal Medicinemeriatmaja100% (1)
- HypertensioninPregnancy ACOGDocument100 pagesHypertensioninPregnancy ACOGIssac RojasNo ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- Literature Review of Hypertension in PregnancyDocument7 pagesLiterature Review of Hypertension in Pregnancyc5jbmre7100% (1)
- البحث aziz alhaidariDocument51 pagesالبحث aziz alhaidariabdulaziz saif ali mansoorNo ratings yet
- The Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDocument15 pagesThe Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDaniela UrreaNo ratings yet
- Presenter DR - Sachin Shekde (Assistant DHO) Guide DR - Yogesh ManeDocument37 pagesPresenter DR - Sachin Shekde (Assistant DHO) Guide DR - Yogesh Maneymane7461No ratings yet
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyFrom EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNo ratings yet
- Pregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervalDocument3 pagesPregnancy Following Miscarriage What Is The Optimum Interpregnancy IntervallcmurilloNo ratings yet
- Obgm Feb2018 Vol.30 No.2 PDFDocument55 pagesObgm Feb2018 Vol.30 No.2 PDFlcmurilloNo ratings yet
- Everyday Contraception ConsiderationsDocument15 pagesEveryday Contraception ConsiderationslcmurilloNo ratings yet
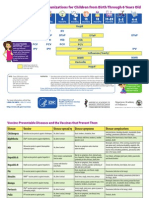
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrslcmurilloNo ratings yet
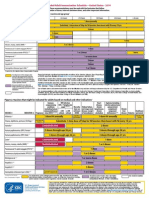
- Catchup Schedule BWDocument4 pagesCatchup Schedule BWlcmurilloNo ratings yet
- Adult Schedule 11x17Document2 pagesAdult Schedule 11x17lcmurilloNo ratings yet
- Adult ScheduleDocument3 pagesAdult SchedulelcmurilloNo ratings yet
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloNo ratings yet
- Fetal DistressDocument48 pagesFetal DistressLenny SucalditoNo ratings yet
- PCM Activity - Abella, Franz KarlDocument2 pagesPCM Activity - Abella, Franz KarlFranz AbellaNo ratings yet
- 1 Chapter 21 Pregnancy Complication BLEEDING DURING PREGNANCYDocument76 pages1 Chapter 21 Pregnancy Complication BLEEDING DURING PREGNANCYCAÑADA, JOHANNELYN M.No ratings yet
- A Review On The Oral Health of Pregnant Women Provided With Basic Oral Health Care (BOHC) in The Province of Davao Oriental: A Local PerspectiveDocument17 pagesA Review On The Oral Health of Pregnant Women Provided With Basic Oral Health Care (BOHC) in The Province of Davao Oriental: A Local PerspectiveAudrey Kristina MaypaNo ratings yet
- Parmed Xpreg PDFDocument4 pagesParmed Xpreg PDFriddhiNo ratings yet
- Case Study P.TDocument5 pagesCase Study P.TSharon WilliamsNo ratings yet
- Antenatalcare CPG SlideDocument62 pagesAntenatalcare CPG SlideAdam ChungNo ratings yet
- Utero Re Laks AnDocument8 pagesUtero Re Laks AnInce NurfiantyNo ratings yet
- Introduction To Community Health 7th Edition Mckenzie Test BankDocument38 pagesIntroduction To Community Health 7th Edition Mckenzie Test Bankhudsoncolepiu100% (17)
- Pregnancy Planning, Smoking BeDocument8 pagesPregnancy Planning, Smoking BeRita NoviantiNo ratings yet
- @medicalbookpdf Preeclampsia PDFDocument286 pages@medicalbookpdf Preeclampsia PDFgalihsupanji111_2230No ratings yet
- Fetal Inflamatory Response SyndromeDocument9 pagesFetal Inflamatory Response SyndromeAnonymous mvNUtwidNo ratings yet
- An Approach To The Management of Hyperbilirubinemia in The Preterm Infant Less Than 35 Weeks of GestationDocument5 pagesAn Approach To The Management of Hyperbilirubinemia in The Preterm Infant Less Than 35 Weeks of Gestationberthad33No ratings yet
- What Is Sexual and Reproductive Health Promotion What Are Sexual Health Issues How Sexual and Reproductive Health Status Can Be ImprovedDocument4 pagesWhat Is Sexual and Reproductive Health Promotion What Are Sexual Health Issues How Sexual and Reproductive Health Status Can Be ImprovedIJARP PublicationsNo ratings yet
- Journal Hydramnios PDFDocument10 pagesJournal Hydramnios PDFMoh RamliNo ratings yet
- Seminar Onlabour and Complicaton1Document5 pagesSeminar Onlabour and Complicaton1PriyaNo ratings yet
- INTRODUCTIONDocument3 pagesINTRODUCTIONSoumya Suguna TripathyNo ratings yet
- Non Invasive Versus Invasive Respiratory Support in Preterm InfantsDocument25 pagesNon Invasive Versus Invasive Respiratory Support in Preterm InfantshosnameskarNo ratings yet
- Final Exam NCM 109. NotesDocument18 pagesFinal Exam NCM 109. Noteskenken the Explorer0% (1)
- Articulo Hernia OriginalDocument7 pagesArticulo Hernia OriginalmelvaNo ratings yet
- Introduction To Community Health 7th Edition Mckenzie Test BankDocument11 pagesIntroduction To Community Health 7th Edition Mckenzie Test Banksinhhanhi7rp100% (35)
- MS GuldaneDocument22 pagesMS GuldaneKhyy SafitryNo ratings yet
- Pitfalls, Problems, and Progress in Bronchopulmonary DysplasiaDocument14 pagesPitfalls, Problems, and Progress in Bronchopulmonary Dysplasiatrixie2k7No ratings yet
- 1.causes For Neonatal Sepsis, Newborn Sepsis, Neonatal Infection, Sepsis TreatmentDocument12 pages1.causes For Neonatal Sepsis, Newborn Sepsis, Neonatal Infection, Sepsis TreatmentlardiyahNo ratings yet
- Bacteriuria Asintomática & Embarazo - Smaill 2007Document12 pagesBacteriuria Asintomática & Embarazo - Smaill 2007Rolando LaraNo ratings yet
- Recommendations To Prevent and Control Iron Deficiency in The United StatesDocument28 pagesRecommendations To Prevent and Control Iron Deficiency in The United StatesAndiFitryanaNo ratings yet
- Bleeding DisorderDocument5 pagesBleeding DisorderAgnes MelayNo ratings yet
- Centile ChartsDocument20 pagesCentile ChartsJames DaviesNo ratings yet
- Soal SoalDocument17 pagesSoal SoalflorensiaNo ratings yet