You might also like
- Udan ConceptsDocument2 pagesUdan ConceptsLheidaniel MMM.100% (5)
- Nclex Past QuestionsDocument452 pagesNclex Past Questionsjyka100% (21)
- Management of Patients On Systemic Steroids - An Oral Surgery PerspectiveDocument7 pagesManagement of Patients On Systemic Steroids - An Oral Surgery PerspectiveMohammad Abdulmon’emNo ratings yet
- Pentagon NLE Review NotesDocument33 pagesPentagon NLE Review NotesChieChay Dub93% (123)
- Psych Nursing Complete Edited Royal PentagonDocument32 pagesPsych Nursing Complete Edited Royal PentagonRichard Ines Valino100% (68)
- Pentagon Notes PALMERDocument27 pagesPentagon Notes PALMERPaula100% (3)
- Review Notes in Pharmacology - NCLEXDocument1 pageReview Notes in Pharmacology - NCLEXLalaine April E. Ortiola79% (29)
- Nursing Jurisprudence ReviewDocument6 pagesNursing Jurisprudence Reviewɹǝʍdןnos96% (28)
- Pediatric Nursing ReviewDocument45 pagesPediatric Nursing Reviewɹǝʍdןnos98% (87)
- Childhood Disorders Version of The ScidDocument2 pagesChildhood Disorders Version of The ScidCarmen Spirescu100% (1)
- Palmer Complete Edited Royal PentagonDocument26 pagesPalmer Complete Edited Royal PentagonRichard Ines Valino98% (42)
- Nursing Research: Pentagon Professional Adjustment, Legal Management, Ethics & Research in NursingDocument27 pagesNursing Research: Pentagon Professional Adjustment, Legal Management, Ethics & Research in NursingMellisa Faith Yebes GoNo ratings yet
- Fundamentals of Nursing Bullets (Nle & Nclex)Document47 pagesFundamentals of Nursing Bullets (Nle & Nclex)Richard Ines Valino100% (36)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Abpsych Barlow Reviewer 1 Abpsych Barlow Reviewer 1Document30 pagesAbpsych Barlow Reviewer 1 Abpsych Barlow Reviewer 1Sharemax Holdings, Inc.No ratings yet
- Pentagon Reviewer Med SurgDocument31 pagesPentagon Reviewer Med SurgKathy Real VillsNo ratings yet
- Communicable Dse ReviewerDocument13 pagesCommunicable Dse ReviewerRichard Ines Valino100% (29)
- Maternity Nursing Edited Royal PentagonDocument49 pagesMaternity Nursing Edited Royal PentagonRichard Ines Valino95% (38)
- Nle TipsDocument4 pagesNle Tipskajama_62896% (28)
- Nursing Board Exam ReviewerDocument32 pagesNursing Board Exam ReviewerRose Anne Mückl100% (9)
- RNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2Document4 pagesRNSG 1533 Raising The Bar For Success Concept: Metabolism: Diabetes Type 1/diabetes Type 2katrinasdNo ratings yet
- Community Health Nursing Practice Questions With RationalesDocument15 pagesCommunity Health Nursing Practice Questions With RationalesFelice Lamzon Labrador100% (2)
- Maternity Nursing Edited Royal PentagonDocument49 pagesMaternity Nursing Edited Royal PentagonRichard Ines Valino95% (38)
- ACUTE AND CHRONIC PANCREATITIS-undoneDocument6 pagesACUTE AND CHRONIC PANCREATITIS-undonecory kurdapyaNo ratings yet
- Tips On NURSING LICENSURE EXAMDocument4 pagesTips On NURSING LICENSURE EXAMFernando Maglunob Lastrollo Jr.94% (17)
- Nle Tips MS PDFDocument11 pagesNle Tips MS PDFjthsNo ratings yet
- The Royal Pentagon Review Specialist Inc. Pediatric NursingDocument55 pagesThe Royal Pentagon Review Specialist Inc. Pediatric NursingDavid PunzalanNo ratings yet
- Nursing Board Exam ReviewerDocument32 pagesNursing Board Exam ReviewerGan BangNo ratings yet
- Pentagon ReviewDocument33 pagesPentagon ReviewRaissa Jane Sariana Bino100% (2)
- Nle Pentagon Reviewer For Nclex Answer QuestionsDocument30 pagesNle Pentagon Reviewer For Nclex Answer QuestionsSpoonNo ratings yet
- DEAR TO NCLEX's HEART PDFDocument452 pagesDEAR TO NCLEX's HEART PDFrn msn100% (4)
- Nle ms1Document32 pagesNle ms1Neil AlviarNo ratings yet
- Emergency Room: Case Scenario (Group 1)Document40 pagesEmergency Room: Case Scenario (Group 1)Victoria Castillo TamayoNo ratings yet
- Pediatric EmergencyDocument98 pagesPediatric Emergencyian ismail100% (5)
- Emergency Medicine: Questions & AnswersDocument83 pagesEmergency Medicine: Questions & AnswersDev Yadav100% (2)
- Nclex BulletsDocument34 pagesNclex Bulletssaroberts2202100% (1)
- Neurologic NursingDocument14 pagesNeurologic Nursingtheglobalnursing100% (6)
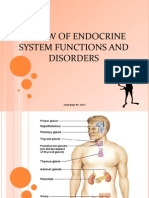
- Review of Endocrine System Functions and Disorders: Arnel Ipapo RN, MANDocument51 pagesReview of Endocrine System Functions and Disorders: Arnel Ipapo RN, MANcha_cha_magistradoNo ratings yet
- Pediatric NursingDocument14 pagesPediatric NursingJoanne PaulineNo ratings yet
- CC 2 Mei 2017 PneumoniaDocument37 pagesCC 2 Mei 2017 PneumoniaAhimsa Yoga AninditaNo ratings yet
- Care Plan 1 Med SurgeDocument25 pagesCare Plan 1 Med Surgeania ojedaNo ratings yet
- CMS Family Medicine Form: Cluster HeadacheDocument4 pagesCMS Family Medicine Form: Cluster HeadacheAnnaNo ratings yet
- HypertensionDocument38 pagesHypertensionmariatheressamercadoNo ratings yet
- Nurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Document27 pagesNurul Ilmi Hajar (PO.71.3.201.14.1.130) Nurul Khabliana (PO.71.3.201.14.1.131)Nurulilmi hajarNo ratings yet
- AGN 3B FinalDocument37 pagesAGN 3B FinalKristine Dela CruzNo ratings yet
- Case Report: A 51 - Year Old Male Presented With Shortness of BreathDocument24 pagesCase Report: A 51 - Year Old Male Presented With Shortness of BreathAlisya NadhilahNo ratings yet
- Department of Cardiology Dr. Md. Abu Faisal D-Card Student DMCHDocument32 pagesDepartment of Cardiology Dr. Md. Abu Faisal D-Card Student DMCHKunwar Sidharth SaurabhNo ratings yet
- Case Study Jim SandersonDocument6 pagesCase Study Jim SandersonJessica McAlexanderNo ratings yet
- Pleural Effusion: Probably Secondary To Parapneumonia ProcessDocument47 pagesPleural Effusion: Probably Secondary To Parapneumonia Processnica tamNo ratings yet
- Elias Fast Hug - Management of The ICU PatientDocument65 pagesElias Fast Hug - Management of The ICU Patientabduljewad arageNo ratings yet
- CABRAL Essential Hypertension Case Presentation and DiscussionDocument9 pagesCABRAL Essential Hypertension Case Presentation and DiscussionCalingalan Hussin CaluangNo ratings yet
- ASD Internship ReportingDocument14 pagesASD Internship ReportingPernel Jose Alam MicuboNo ratings yet
- Syncope: - Selvarathi KDocument27 pagesSyncope: - Selvarathi KSelvarathi KandhaswamyNo ratings yet
- Thomas R. Burklow, MD Asst C., Pediatric Cardiology Walter Reed Army Medical Center National Capital ConsortiumDocument40 pagesThomas R. Burklow, MD Asst C., Pediatric Cardiology Walter Reed Army Medical Center National Capital ConsortiumMuna ZahiraNo ratings yet
- Drugs and It's Indication: Nursing ConsiderationsDocument4 pagesDrugs and It's Indication: Nursing ConsiderationsKenneth NovenoNo ratings yet
- Hypoxic Ischemic Hypoxic Ischemic E HL H E HL H Encephalopathty EncephalopathtyDocument34 pagesHypoxic Ischemic Hypoxic Ischemic E HL H E HL H Encephalopathty EncephalopathtyKatrinaTandoc100% (1)
- Thyroid ParathyroidDocument79 pagesThyroid Parathyroid2M SANCHEZ, CYLESNo ratings yet
- Pediatrics NotesDocument96 pagesPediatrics NotesErwin Jake TagubaNo ratings yet
- IMhpncrisisDocument8 pagesIMhpncrisischaoNo ratings yet
- Birth Asphyxia: by Anne E. Odaro MCM/2017/69852Document26 pagesBirth Asphyxia: by Anne E. Odaro MCM/2017/69852ElvisNo ratings yet
- Pediatric Anaphylaxis: Pediatric Stage Faculty of Medicine Christian University of Indonesia 23 September - 16 NovemberDocument34 pagesPediatric Anaphylaxis: Pediatric Stage Faculty of Medicine Christian University of Indonesia 23 September - 16 NovemberNovelia CarolinNo ratings yet
- Psychosis Due To Endocrine DISTURBANCESDocument47 pagesPsychosis Due To Endocrine DISTURBANCESmr_davidNo ratings yet
- CVA NotesDocument21 pagesCVA NotesVaibhav BhatiaNo ratings yet
- HipotiroidDocument27 pagesHipotiroidJuwitaNo ratings yet
- Congestive Heart Failure ThesisDocument8 pagesCongestive Heart Failure ThesisAshley Smith100% (2)
- PROCEDUREDocument10 pagesPROCEDURESabrina ReyesNo ratings yet
- Winter 2024 Medical TrainingDocument57 pagesWinter 2024 Medical Trainingapi-125557135No ratings yet
- Medical Surgical Nursing Bullets Nle NclexDocument95 pagesMedical Surgical Nursing Bullets Nle NclexRichard Ines Valino100% (2)
- Psychiatric Nursing Bullets (Nle & Nclex)Document21 pagesPsychiatric Nursing Bullets (Nle & Nclex)Richard Ines Valino100% (24)
- Maternal & Child Nursing Bullets (Nle & Nclex)Document38 pagesMaternal & Child Nursing Bullets (Nle & Nclex)Richard Ines Valino95% (22)
- Maternity NursingDocument28 pagesMaternity Nursingja100% (11)
- Nursing Practice II EdgeworthDocument9 pagesNursing Practice II EdgeworthRichard Ines Valino100% (1)
- Nursing Practice V EdgeworthDocument8 pagesNursing Practice V EdgeworthRichard Ines Valino100% (8)
- Medical Surgical NursingDocument35 pagesMedical Surgical Nursingja98% (40)
- Nursing Practice IV EdgeworthDocument9 pagesNursing Practice IV EdgeworthRichard Ines Valino100% (6)
- MS Review EdgeworthDocument89 pagesMS Review EdgeworthRichard Ines Valino100% (7)
- Nursing Practice III EdgeworthDocument8 pagesNursing Practice III EdgeworthRichard Ines Valino100% (5)
- COPAR ReviewerDocument6 pagesCOPAR ReviewerRichard Ines Valino94% (16)
- Nursing Practice I EdgeworthDocument8 pagesNursing Practice I EdgeworthRichard Ines Valino100% (5)
- Physical AssessmentDocument3 pagesPhysical AssessmentRichard Ines Valino100% (6)
- Therapeutic DietsDocument8 pagesTherapeutic DietsmArLoN91% (11)
- Surgical InstrumentsDocument8 pagesSurgical InstrumentsSharmaine Simon91% (11)
- Medical AbbreviationsDocument30 pagesMedical AbbreviationsRichard Ines Valino100% (10)
- IMCIDocument51 pagesIMCIkhyzyrNo ratings yet
- Community Organizing Participatory Action ResearchDocument5 pagesCommunity Organizing Participatory Action ResearchRichard Ines Valino100% (6)
- Normal NewbornDocument22 pagesNormal NewbornRichard Ines Valino100% (6)
- AntidotesDocument1 pageAntidotesRichard Ines Valino100% (6)
- Read Questions Carefully: No, Except, and None. Answers Containing These Key Word Are Rarely Correct Because TheyDocument4 pagesRead Questions Carefully: No, Except, and None. Answers Containing These Key Word Are Rarely Correct Because TheyRichard Ines Valino100% (6)
- Anti Psychotic DrugsDocument2 pagesAnti Psychotic DrugscalfornianursingacadNo ratings yet
- NCM 107 Skills Module MCN PDFDocument18 pagesNCM 107 Skills Module MCN PDFmysterioushumane100% (2)
- Forbidden Secrets From Nature's Pharmacy To Reverse Diabetes and Blood Sugar ProblemsDocument54 pagesForbidden Secrets From Nature's Pharmacy To Reverse Diabetes and Blood Sugar Problemsa1khanNo ratings yet
- Intussusception: PathophysiologyDocument8 pagesIntussusception: PathophysiologyNaufal AndaluNo ratings yet
- Immunity and Vaccines As Biology Answers AQA OCR EdexcelDocument3 pagesImmunity and Vaccines As Biology Answers AQA OCR EdexcelShela HuangNo ratings yet
- Carpal Tunnel SyndromeDocument3 pagesCarpal Tunnel SyndromeAvery SandsNo ratings yet
- Science 2005 Badman 1909 14Document7 pagesScience 2005 Badman 1909 14Pejvak KHorram DinNo ratings yet
- Sexual Dysfunction 3Document23 pagesSexual Dysfunction 3Wael GaberNo ratings yet
- Candida ProtocolDocument9 pagesCandida Protocolabazan100% (2)
- Q1. A. Describe EPI Program of Pakistan?Document3 pagesQ1. A. Describe EPI Program of Pakistan?Abdul MominNo ratings yet
- M-Protocol For MGMT of Pregab-Gaba SussexDocument2 pagesM-Protocol For MGMT of Pregab-Gaba SussexMatias IglesiasNo ratings yet
- All Gone: A Memoir of My Mother's Dementia With Refreshments by Alex WitchelDocument4 pagesAll Gone: A Memoir of My Mother's Dementia With Refreshments by Alex WitchelSouthern California Public RadioNo ratings yet
- The Obsolescence of Formocresol: B. LewisDocument4 pagesThe Obsolescence of Formocresol: B. LewisAlan Vargas100% (1)
- Recognizing A Technically Adequate Chest X-RayDocument30 pagesRecognizing A Technically Adequate Chest X-Rayachmad rizkiNo ratings yet
- Readiness Assessment Tools - CAVITE PROVINCE 2023 MR SIA - (PHO CHO MHO RHU HC BHSDocument186 pagesReadiness Assessment Tools - CAVITE PROVINCE 2023 MR SIA - (PHO CHO MHO RHU HC BHSChristean Val Bayani ValezaNo ratings yet
- Nursing ProcedureDocument240 pagesNursing ProcedurerainNo ratings yet
- Makalah Bahasa InggrisDocument11 pagesMakalah Bahasa Inggrismei diana sara'isNo ratings yet
- Laser SafetyDocument3 pagesLaser SafetyEbaa BarghouthiNo ratings yet
- Introduction To Cleft Lip and Palate: Prof. Adetokunbo Adebola Aminu Kano TH / Bayero University, Kano, NigeriaDocument9 pagesIntroduction To Cleft Lip and Palate: Prof. Adetokunbo Adebola Aminu Kano TH / Bayero University, Kano, NigeriaYuan MarcelitaNo ratings yet
- Pharma Syllabus (Edited)Document21 pagesPharma Syllabus (Edited)BSN CMUNo ratings yet
- Jurnal PDPH Anest RisaDocument15 pagesJurnal PDPH Anest Risaadit rifqiNo ratings yet
- Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)Document52 pagesChronic Inflammatory Demyelinating Polyneuropathy (CIDP)Sudu manike ManikNo ratings yet
- 8B - Spondylolysis, SpondylolisthesisDocument14 pages8B - Spondylolysis, SpondylolisthesismorlaszloNo ratings yet
- Parkinsonism and Related DisordersDocument7 pagesParkinsonism and Related DisordersnellieauthorNo ratings yet
- Microscopic-Exam TODO NADocument78 pagesMicroscopic-Exam TODO NAlily beautyNo ratings yet
- Mutu Farmasi Jan 24Document9 pagesMutu Farmasi Jan 24Fenny Aliska Larasaty WijayaNo ratings yet
- The Comorbidities of Dysmenorrhea: A Clinical Survey Comparing Symptom Profile in Women With and Without EndometriosisDocument14 pagesThe Comorbidities of Dysmenorrhea: A Clinical Survey Comparing Symptom Profile in Women With and Without EndometriosisSeptian WidiantoNo ratings yet