You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
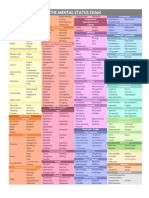
- Mse Cheat Sheet - Us Letter (Printable)Document1 pageMse Cheat Sheet - Us Letter (Printable)Ai Hwa Lim100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Foundations of Forensic Mental Health Assessment PDFDocument193 pagesFoundations of Forensic Mental Health Assessment PDFZACHARIAH MANKIRNo ratings yet
- Psychological First AidDocument51 pagesPsychological First AidDivh Boquecoz100% (13)
- Kring Abnormal Psychology Chapter 5 Mood Disorders NotesDocument14 pagesKring Abnormal Psychology Chapter 5 Mood Disorders NotesAnn Ross FernandezNo ratings yet
- Parenting StylesDocument5 pagesParenting Stylesapi-411652403No ratings yet
- CHC33015-Sub 1 Assessment PDFDocument87 pagesCHC33015-Sub 1 Assessment PDFMaimuna100% (1)
- Behaviour Therapy NotesDocument2 pagesBehaviour Therapy NotesPrathamanantaNo ratings yet
- What Is Disorganized Schizophrenia (Hebephrenia) - What Causes Disorganized Schizophrenia - Medical News TodayDocument7 pagesWhat Is Disorganized Schizophrenia (Hebephrenia) - What Causes Disorganized Schizophrenia - Medical News TodayYlmi Aridah KhaeraNo ratings yet
- Jose Catalan - Mental Health and HIV Infection (Social Aspect of Aids Series) (1999) PDFDocument254 pagesJose Catalan - Mental Health and HIV Infection (Social Aspect of Aids Series) (1999) PDFManuelNo ratings yet
- Rowe and Kahn's Model of Successful AgingDocument8 pagesRowe and Kahn's Model of Successful AgingJuly Prieto MarinNo ratings yet
- The Dave Elman InductionDocument6 pagesThe Dave Elman InductionDealer RamarayoNo ratings yet
- Behavioural Problems Among School Going ChildrenDocument5 pagesBehavioural Problems Among School Going ChildrenAnonymous izrFWiQNo ratings yet
- CHN Therioes&models FinalDocument29 pagesCHN Therioes&models Finalkuruvagadda sagarNo ratings yet
- Jensen DossDocument3 pagesJensen DossjlbermudezcNo ratings yet
- Regular Article: Psychiatry and Clinical Neurosciences (2002), 56, 41-53Document13 pagesRegular Article: Psychiatry and Clinical Neurosciences (2002), 56, 41-53DiLaa 'cendawa' AzwaniieNo ratings yet
- World Psychiatry - 2024 - Schramm - Algorithm Based Modular Psychotherapy Vs Cognitive Behavioral Therapy For PatientsDocument10 pagesWorld Psychiatry - 2024 - Schramm - Algorithm Based Modular Psychotherapy Vs Cognitive Behavioral Therapy For PatientsRodrigo HerNo ratings yet
- Cornell Notes Sheet: 1.) What Is Mental Health?Document4 pagesCornell Notes Sheet: 1.) What Is Mental Health?Aleena Mariya SebastianNo ratings yet
- Einstein 2004Document11 pagesEinstein 2004Stefania PDNo ratings yet
- Pediatric Rehabilitation: The ICF-CY Model As Concept For TreatmentDocument2 pagesPediatric Rehabilitation: The ICF-CY Model As Concept For TreatmentAtet KurniadiNo ratings yet
- Psychiatric Nursing ProcessDocument24 pagesPsychiatric Nursing ProcessJoric MagusaraNo ratings yet
- Expression and Regulation of SadnessDocument77 pagesExpression and Regulation of SadnessDimitra KlouvatouNo ratings yet
- Shyness & Anxiety: A Review of LiteratureDocument8 pagesShyness & Anxiety: A Review of Literatureapi-285426523No ratings yet
- Additional Info For SchizophreniaDocument11 pagesAdditional Info For SchizophreniaJasmin JacobNo ratings yet
- Chapter 8 QuestionsDocument2 pagesChapter 8 QuestionsMorganNo ratings yet
- W6L28Document16 pagesW6L28N SinghNo ratings yet
- Teacher Beliefs and Stress JRECBTDocument17 pagesTeacher Beliefs and Stress JRECBTandreea_zgrNo ratings yet
- Choice and Medication Benefits LeafletDocument3 pagesChoice and Medication Benefits LeafletrowanpurdyNo ratings yet
- Definition of Youth ViolenceDocument4 pagesDefinition of Youth ViolenceMoniciaTopatopBrooksOkNo ratings yet
- Guns, Scalpels, and Sutures: The Cost of Gunshot Wounds in Children and AdolescentsDocument11 pagesGuns, Scalpels, and Sutures: The Cost of Gunshot Wounds in Children and Adolescentsyoanutami putrisinagaNo ratings yet
- Mental Health Exercises For ReviewDocument6 pagesMental Health Exercises For ReviewKarson22No ratings yet