You might also like
- Iron Deficiency Anemia OkDocument54 pagesIron Deficiency Anemia OkRamsha ZafarNo ratings yet
- Capstone Project FileDocument48 pagesCapstone Project FileParveen KumarNo ratings yet
- Eries: 6.0 TO 8.0 TONDocument12 pagesEries: 6.0 TO 8.0 TONNos GoteNo ratings yet
- Zero Carbon Building StandardsDocument32 pagesZero Carbon Building Standardsjoslinmtg100% (1)
- Metabolic Syndrome Is Related Cardio-Cerebro Vascular DiseaseDocument40 pagesMetabolic Syndrome Is Related Cardio-Cerebro Vascular DiseaseSatya FitriansyahNo ratings yet
- Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument18 pagesDr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik Unjariska yulizaNo ratings yet
- Strategies For HarvestDocument86 pagesStrategies For HarvestBeka AsraNo ratings yet
- Interpretasi Urine RutinDocument118 pagesInterpretasi Urine Rutinboy jendri huluNo ratings yet
- Von Willebrand DiseaseDocument14 pagesVon Willebrand DiseaseCsn VittalNo ratings yet
- Adrenal Disease VTCDocument50 pagesAdrenal Disease VTCElena Borş Morari100% (1)
- ANEMIADocument28 pagesANEMIAwanda0% (1)
- Leaflet DislipidemiaDocument2 pagesLeaflet DislipidemiaRskia Arvita BundaNo ratings yet
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Krisis Hipertensi SWEIM 2017 DR Chandra IrwanadiDocument49 pagesKrisis Hipertensi SWEIM 2017 DR Chandra IrwanadiDebby Christiana SNo ratings yet
- Irritable Bowel Syndrome (Ibs)Document9 pagesIrritable Bowel Syndrome (Ibs)EmeraldyModyNo ratings yet
- APO SNP Training - GlanceDocument78 pagesAPO SNP Training - GlanceAshwani SharmaNo ratings yet
- Ryan Ronquillo ComplaintDocument39 pagesRyan Ronquillo ComplaintMichael_Lee_RobertsNo ratings yet
- The Hepatorenal SyndromeDocument26 pagesThe Hepatorenal SyndromeWaraBawanaNo ratings yet
- Revised PPT Obesitas Anak FitriaDocument22 pagesRevised PPT Obesitas Anak FitriaFitri RahmawatiNo ratings yet
- Dislipidemia: Prof. Dr. WH. Sibuea, SP - PDDocument37 pagesDislipidemia: Prof. Dr. WH. Sibuea, SP - PDandinarang0% (1)
- Smart AntennasDocument40 pagesSmart AntennasMeeraNo ratings yet
- Advance Care Planning English VersionDocument9 pagesAdvance Care Planning English VersionAlma NurfitriaNo ratings yet
- INSULIN Dan Obat Hipoglikemik OralDocument35 pagesINSULIN Dan Obat Hipoglikemik OralSwietenia Rambu SabatiNo ratings yet
- HypoalbuminemiaDocument1 pageHypoalbuminemiaMunish DograNo ratings yet
- n378.008 Iris Website Staging of CKD PDFDocument8 pagesn378.008 Iris Website Staging of CKD PDFrutebeufNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Hipertensi JNC 8Document7 pagesHipertensi JNC 8Elisse StephanieNo ratings yet
- Nilai Lab NormalDocument3 pagesNilai Lab Normalraa_zhraNo ratings yet
- Diagnosis Dan Diagnosis Banding DM SK 2Document99 pagesDiagnosis Dan Diagnosis Banding DM SK 2syahron maskatNo ratings yet
- FINAL Management Update of Hyperuricemia & GoutDocument50 pagesFINAL Management Update of Hyperuricemia & GoutNeni Septria NingsihNo ratings yet
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Document46 pages1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริNo ratings yet
- Nutrisi Makro GeriatriDocument28 pagesNutrisi Makro Geriatrieka suprapti100% (1)
- Henoch Schönlein PurpuraDocument12 pagesHenoch Schönlein PurpuraRavania Rahadian Putri100% (1)
- IPD - Nutrition Elderly enDocument26 pagesIPD - Nutrition Elderly ensolgraNo ratings yet
- HIPERTENSI Dan Penyakit KardiovaskularDocument39 pagesHIPERTENSI Dan Penyakit KardiovaskulardhestiNo ratings yet
- Daftar Pustaka Hipertensi Pada Usia MudaDocument10 pagesDaftar Pustaka Hipertensi Pada Usia MudaToby Hadinata WiranegaraNo ratings yet
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- Slide Chronic Pain-Rudy Hidayat-Iai PDFDocument30 pagesSlide Chronic Pain-Rudy Hidayat-Iai PDFAsri ArrachmanNo ratings yet
- Medical Check Up: Cek KesehatanDocument20 pagesMedical Check Up: Cek KesehatanEmi PephiNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- MAA Ossoral DexaDocument33 pagesMAA Ossoral DexaDitaAnggaraKusumaNo ratings yet
- Aquamin Human Trials Overview 15102015Document17 pagesAquamin Human Trials Overview 15102015May Juin LeeNo ratings yet
- Peresepan OlahragaDocument7 pagesPeresepan OlahragaAngga Julyananda PradanaNo ratings yet
- DyslipidemiaDocument21 pagesDyslipidemiaBasil HussamNo ratings yet
- Anemia: Dr. Saranya VinothDocument45 pagesAnemia: Dr. Saranya Vinothareeb khanNo ratings yet
- Reaksi AnafilaksisDocument34 pagesReaksi AnafilaksisPutri Reno IntanNo ratings yet
- Manajemen HipertensiDocument46 pagesManajemen HipertensiYeni BelawatiNo ratings yet
- A Case of Aplastic Anemia With Crbsi in EsrfDocument45 pagesA Case of Aplastic Anemia With Crbsi in EsrfRidhwan Hakim ZainurinNo ratings yet
- Naskah Publikasi LansiaDocument17 pagesNaskah Publikasi LansiaVhiny ChaNo ratings yet
- AHA Hypertension JournalDocument10 pagesAHA Hypertension JournalTiwi QiraNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- Tata Laksana TB MDR Dr. PrayudiDocument58 pagesTata Laksana TB MDR Dr. PrayudiDeaNo ratings yet
- Dosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDocument1 pageDosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDenny RamdhanNo ratings yet
- Antihyperglycemic Agents Comparison ChartDocument9 pagesAntihyperglycemic Agents Comparison ChartBonnieNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- Alifa Nasyahta Rosiana 22010110110055 Bab8KTIDocument49 pagesAlifa Nasyahta Rosiana 22010110110055 Bab8KTIYudhi SetiabudiNo ratings yet
- Atherosclerosis & Trombosis Dr. FaturochmanDocument50 pagesAtherosclerosis & Trombosis Dr. FaturochmanPutry RizqiaNo ratings yet
- COVID-19 Weekly Epidemiological Update: Global OverviewDocument31 pagesCOVID-19 Weekly Epidemiological Update: Global OverviewPaolaNo ratings yet
- Postmortem Biochemistry of Vitreous Humor and Glucose MetabolismDocument7 pagesPostmortem Biochemistry of Vitreous Humor and Glucose MetabolismsbeyeforhireNo ratings yet
- Hipertiroid HarrisonDocument8 pagesHipertiroid HarrisonravenskaNo ratings yet
- Flunarizine HCL PDFDocument76 pagesFlunarizine HCL PDFo cindy glaudiaNo ratings yet
- Legacy Effect in Diabetes MnanagementDocument9 pagesLegacy Effect in Diabetes MnanagementSouradipta GangulyNo ratings yet
- Albumin in Liver Cirrhosis, SADocument37 pagesAlbumin in Liver Cirrhosis, SADwinita ViviantiNo ratings yet
- Teori Obat DispepsiaDocument13 pagesTeori Obat DispepsiaPasti SuksesNo ratings yet
- Physiology AlbuminDocument5 pagesPhysiology AlbuminDoc HamsNo ratings yet
- The Colloid ControversyDocument11 pagesThe Colloid ControversyAlessandra SantanaNo ratings yet
- Controversias en AlbuminaDocument14 pagesControversias en Albuminajesus_berber_2No ratings yet
- 00C PrefaceDocument2 pages00C PrefaceJessica AdvínculaNo ratings yet
- Leprosy LancetDocument11 pagesLeprosy LancetJessica AdvínculaNo ratings yet
- 00B Forthcoming IssuesDocument1 page00B Forthcoming IssuesJessica AdvínculaNo ratings yet
- Diabetic Foot Infections A Team-Oriented Review of Medical and Surgical ManagementDocument7 pagesDiabetic Foot Infections A Team-Oriented Review of Medical and Surgical ManagementJessica AdvínculaNo ratings yet
- Consensus Development in Acute Renal Failure The Acute Dialysis Quality InitiativeDocument6 pagesConsensus Development in Acute Renal Failure The Acute Dialysis Quality InitiativeJessica AdvínculaNo ratings yet
- Acute Kidney Injury LANCETDocument11 pagesAcute Kidney Injury LANCETJessica AdvínculaNo ratings yet
- Bronchiolitis in Children: Scottish Intercollegiate Guidelines NetworkDocument46 pagesBronchiolitis in Children: Scottish Intercollegiate Guidelines NetworkAnonymous 6iwMFwNo ratings yet
- Nutrition & Wound Care: Christina Merryfield, Lead Dietitian, Bupa Cromwell HospitalDocument4 pagesNutrition & Wound Care: Christina Merryfield, Lead Dietitian, Bupa Cromwell HospitalhafiezAmandaNo ratings yet
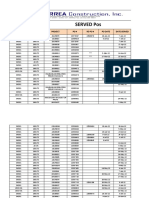
- Served POsDocument21 pagesServed POsYay DumaliNo ratings yet
- Concrete MixerDocument10 pagesConcrete MixerRafaqat NiaziNo ratings yet
- Conservation Awareness and Techniques in Buluan Lake, Maguindanao, BARMMDocument9 pagesConservation Awareness and Techniques in Buluan Lake, Maguindanao, BARMMPsychology and Education: A Multidisciplinary JournalNo ratings yet
- TA202A - Manufacturing Processes II Machining Processes and MachinesDocument16 pagesTA202A - Manufacturing Processes II Machining Processes and Machinesprashant vermaNo ratings yet
- Automated Sand Gravity Sand Filter SystemDocument58 pagesAutomated Sand Gravity Sand Filter SystemMichaelNo ratings yet
- Costing of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMDocument3 pagesCosting of Sea Water RO Plant KPT Manora Design at 100,000 IGPD at 35,000 PPMMohtashim KazmiNo ratings yet
- Potential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334Document6 pagesPotential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334DicksonNo ratings yet
- ESL Mid Test Semester 1 Grade 3Document3 pagesESL Mid Test Semester 1 Grade 3Elis ElisNo ratings yet
- LATsol SMAN 57Document10 pagesLATsol SMAN 57NAYLA NURRIZKYNo ratings yet
- 32LS3400 KoreaDocument60 pages32LS3400 KoreaNightin VargheseNo ratings yet
- Appendix 1: Apmoption Apm3Rdpar CsotpmDocument8 pagesAppendix 1: Apmoption Apm3Rdpar CsotpmromixrayzenNo ratings yet
- Penn State Emergency Residency Conference APRIL 2023Document10 pagesPenn State Emergency Residency Conference APRIL 2023jhk0428No ratings yet
- Burroughs Jungle Tales of TarzanDocument133 pagesBurroughs Jungle Tales of Tarzanfr1z1derNo ratings yet
- HW 7Document3 pagesHW 7Khuram MaqsoodNo ratings yet
- EIHA-THC Levels in Hemp FoodDocument3 pagesEIHA-THC Levels in Hemp FoodMichal TőzsérNo ratings yet
- I. Annex 1: Specific Requirements For SurveysDocument3 pagesI. Annex 1: Specific Requirements For SurveysSubhadip BairiNo ratings yet
- Anatomy of A FireworkDocument4 pagesAnatomy of A FireworkMuthu KumarNo ratings yet
- Student Exploration: HomeostasisDocument3 pagesStudent Exploration: HomeostasisJordan TorresNo ratings yet
- Sourcing Report - Iffco Olive OilDocument13 pagesSourcing Report - Iffco Olive OilMatheusNo ratings yet
- Power Link Module For LD 800PDocument4 pagesPower Link Module For LD 800PSarah FrazierNo ratings yet
- Vodka and Vanilla Blancmange With Warm RaspberriesDocument6 pagesVodka and Vanilla Blancmange With Warm RaspberriesFranca AkNo ratings yet
- Active Vision-Based Attention Monitoring System FoDocument19 pagesActive Vision-Based Attention Monitoring System FoZaima Sartaj TaheriNo ratings yet