You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ime56350g 2 Felcom15Document51 pagesIme56350g 2 Felcom15SergeyNo ratings yet
- IMAGINEDocument48 pagesIMAGINEGilherme HenriqueNo ratings yet
- The Phantom of The OperaDocument272 pagesThe Phantom of The OperaJames Andrew CurtisNo ratings yet
- V5 Diet ListDocument2 pagesV5 Diet ListRajini KuganasanNo ratings yet
- RoboticsbasicDocument52 pagesRoboticsbasicdanvicNo ratings yet
- Luis J Corona ResumeDocument2 pagesLuis J Corona Resumeapi-337110849No ratings yet
- Phil Precolonial ArtDocument23 pagesPhil Precolonial ArtMonnette Ann Banzuela100% (2)
- CVDocument1 pageCVSiddharth ChauhanNo ratings yet
- Application: Atlanta DWV Sanitary Pipe IsDocument2 pagesApplication: Atlanta DWV Sanitary Pipe IsBruce DoyaoenNo ratings yet
- FAHM 2018 Programme v4Document16 pagesFAHM 2018 Programme v4Aviation Events InternationalNo ratings yet
- Principles of Christian Mental HealthDocument27 pagesPrinciples of Christian Mental HealthMaschil100% (2)
- EUROFOOD Casewhole2Document25 pagesEUROFOOD Casewhole2EL GADROUR EL MEHDINo ratings yet
- ElectronicsDocument6 pagesElectronicsAayush AgrawalNo ratings yet
- XY Plotter V2.0 Laser Engraver Upgrade Pack User Guide MDraw Version 1.0Document41 pagesXY Plotter V2.0 Laser Engraver Upgrade Pack User Guide MDraw Version 1.0franklinNo ratings yet
- Mobile COMPUTINGDocument169 pagesMobile COMPUTINGNPMYS23No ratings yet
- Concrete Construction Article PDF - Quality Control in Concrete ConstructionDocument3 pagesConcrete Construction Article PDF - Quality Control in Concrete ConstructionJeremiah ObiacoroNo ratings yet
- FNN111 Nutrition Chapter 1 NOTES The Role of Nutrition in Our HealthDocument5 pagesFNN111 Nutrition Chapter 1 NOTES The Role of Nutrition in Our HealthRina JungNo ratings yet
- This Study Resource Was: Pas 41 - AgricultureDocument3 pagesThis Study Resource Was: Pas 41 - Agriculturedasha limNo ratings yet
- Group 4: Diet For Healthy Teath BonesDocument26 pagesGroup 4: Diet For Healthy Teath Bonesknowledge chanall chanallNo ratings yet
- School of Natural Sciences Status Report Details School of Natural Sciences Intern's ReportDocument7 pagesSchool of Natural Sciences Status Report Details School of Natural Sciences Intern's ReportAgyao Yam FaithNo ratings yet
- Proline Promass 83 Profibus Dp/Pa: Description of Device FunctionsDocument182 pagesProline Promass 83 Profibus Dp/Pa: Description of Device FunctionsHectorNo ratings yet
- Erd 2 F 005Document1 pageErd 2 F 005Bettina BarrionNo ratings yet
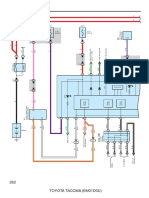
- Combination Meter: 262 Toyota Tacoma (Em01D0U)Document6 pagesCombination Meter: 262 Toyota Tacoma (Em01D0U)hamayunNo ratings yet
- Grade 5 Science Most Essential Learning Competencies MELCsDocument5 pagesGrade 5 Science Most Essential Learning Competencies MELCsPaul Fausto MaghirangNo ratings yet
- The Downward Spiral - RiveraDocument4 pagesThe Downward Spiral - RiveraAnthony AlvaradoNo ratings yet
- 613 Ebce 67 CB 7 DDocument2 pages613 Ebce 67 CB 7 DTheerapong ChansopaNo ratings yet
- Chemistry Revision NotesDocument7 pagesChemistry Revision NotesFarhan RahmanNo ratings yet
- Strategic Marketing AssignmentDocument9 pagesStrategic Marketing Assignmentsaif UllahNo ratings yet
- History of AthleticsDocument30 pagesHistory of AthleticsSTEPHANIE MAGNAYENo ratings yet
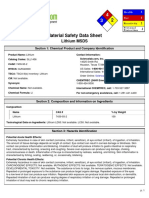
- Msds LiDocument5 pagesMsds Linaren_013No ratings yet