You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Retail Buy & Sell: Can't Ind What You're Looking For? Check Online at Freepressseries - Co.ukDocument4 pagesRetail Buy & Sell: Can't Ind What You're Looking For? Check Online at Freepressseries - Co.ukDigital MediaNo ratings yet
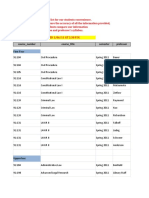
- Course - Number Course - Title Semester Professor: First YearDocument52 pagesCourse - Number Course - Title Semester Professor: First Yearkari262No ratings yet
- Preliminary Design of The Green Diesel Production Process by Hydrotreatment of Vegetable Oils PDFDocument15 pagesPreliminary Design of The Green Diesel Production Process by Hydrotreatment of Vegetable Oils PDFNina KonitatNo ratings yet
- New Lucena National Comprehensive High: SchoolDocument8 pagesNew Lucena National Comprehensive High: Schoolriverastudy01No ratings yet
- Ship's Organizational StructureDocument8 pagesShip's Organizational StructureAmos BagaipoNo ratings yet
- Irradiation of PotatoesDocument26 pagesIrradiation of PotatoesChantre ToiNo ratings yet
- Service Manual LP4235!40!45Document131 pagesService Manual LP4235!40!45assitec9650% (2)
- African Seed Oil PDFDocument14 pagesAfrican Seed Oil PDFAggie QuiNo ratings yet
- English, Science, Mathematics and Health Electromagnetic RadiationDocument3 pagesEnglish, Science, Mathematics and Health Electromagnetic RadiationSofia GabrellaNo ratings yet
- Draft Moa y PvaoDocument5 pagesDraft Moa y PvaoAw LapuzNo ratings yet
- Corporate Tax PlanningDocument18 pagesCorporate Tax PlanningSANDEEP KUMARNo ratings yet
- Chief Architect x6 Users Guide House TutorialDocument40 pagesChief Architect x6 Users Guide House TutorialTrish AntoniNo ratings yet
- JUNOS Network Operations Guide. HardwareDocument722 pagesJUNOS Network Operations Guide. HardwareDmitry MoshkovskyNo ratings yet
- FAQ Partitions and Isolation Groups in SAP CPS by RedwoodDocument2 pagesFAQ Partitions and Isolation Groups in SAP CPS by Redwoodshashidhar thummaNo ratings yet
- Uputstvo Za Medialink by ItlabnetDocument1 pageUputstvo Za Medialink by ItlabnetAsmir DedicNo ratings yet
- Anki Guide For Medical StudentsDocument6 pagesAnki Guide For Medical StudentspchamessNo ratings yet
- Shrink FittingDocument26 pagesShrink FittingmaheshkbandariNo ratings yet
- Cot 2021 Math 3RD Quarter Melc by Sir Ray L. MarasiganDocument3 pagesCot 2021 Math 3RD Quarter Melc by Sir Ray L. MarasiganJennifer Mendoza100% (1)
- Bank Job Recent Questions - Chapter WiseDocument85 pagesBank Job Recent Questions - Chapter Wisetito100% (5)
- Tobacco Pipes Cataloging ManualDocument18 pagesTobacco Pipes Cataloging Manualchippewa05100% (1)
- Perbandingan Respon Hemodinamik 3 Menit Dan 5 Menit Setelah Pemberian Fentanyl 2 MCG/KGBB IV Saat Intubasi Di RSUD DR Saiful Anwar MalangDocument10 pagesPerbandingan Respon Hemodinamik 3 Menit Dan 5 Menit Setelah Pemberian Fentanyl 2 MCG/KGBB IV Saat Intubasi Di RSUD DR Saiful Anwar MalangTigi HereNo ratings yet
- WorkApps ChatDocument18 pagesWorkApps ChatRuletaNo ratings yet
- 616 Roots Ram Whispair Pressure Performance Curve-2Document1 page616 Roots Ram Whispair Pressure Performance Curve-2Mike LongstockNo ratings yet
- Activity 1.1.2 Simple Machines Practice: ProcedureDocument7 pagesActivity 1.1.2 Simple Machines Practice: ProcedureYonjou-Divine VictorinNo ratings yet
- Inner Wheel Club Delhi New EraDocument25 pagesInner Wheel Club Delhi New Eratanvi tanviNo ratings yet
- Pastel Multicolor Gradient Formal Research Paper PresentationDocument29 pagesPastel Multicolor Gradient Formal Research Paper PresentationUmmu NisaNo ratings yet
- Becoming A Cisco Select Certified Partner-Step by Step GuideDocument7 pagesBecoming A Cisco Select Certified Partner-Step by Step Guidemwaseemno181No ratings yet
- Cranfield University: Attempt All QuestionsDocument6 pagesCranfield University: Attempt All QuestionsFabio BosioNo ratings yet
- SS Corrosion SlidesDocument36 pagesSS Corrosion SlidesNathanianNo ratings yet
- Portfolio Performance EvaluationDocument28 pagesPortfolio Performance Evaluationleolau2015No ratings yet